


HEMS & COVID-19

More realistic sim. When using PPE need to consider the time needed to don the equipment and the deficits which might be suffered to dexterity and communication through its usage. Some tasks become difficult when wearing PPE and the difficulties suffered are not intuitive prior to actually simming the scenarios with all stakeholders presence.
The one caveat is that as little PPE should be wasted during this process. In the lead up to Covid19 I witnessed criminal amounts of PPE being wasted during fit testing...
The one caveat is that as little PPE should be wasted during this process. In the lead up to Covid19 I witnessed criminal amounts of PPE being wasted during fit testing...

More realistic sim. When using PPE need to consider the time needed to don the equipment and the deficits which might be suffered to dexterity and communication through its usage. Some tasks become difficult when wearing PPE and the difficulties suffered are not intuitive prior to actually simming the scenarios with all stakeholders presence.
The one caveat is that as little PPE should be wasted during this process. In the lead up to Covid19 I witnessed criminal amounts of PPE being wasted during fit testing...
The one caveat is that as little PPE should be wasted during this process. In the lead up to Covid19 I witnessed criminal amounts of PPE being wasted during fit testing...
With regards to your first point, for all we know this was only one of many ROC drills where they ramped up the "realism" in stages. The next one could have been rotors running to take away the ability to communicate by voice, who knows.
Here is an option to avoid PPE and still protect the pilots, shown here in an AW 139, seems a safe solution to potentially problems?
https://www.heliopsmag.com/chc-based...der-for-aw139A team of CHC engineers, based in Den Helder, Netherlands, has developed and fitted a plastic flexible cockpit/cabin divider that can be fitted to their AW139 fleet.
Highlighting real team work and collaboration between their technical services, maintenance, type technical pilots and management the system has been approved by, Leonardo Helicopters, the CAA-NL and Netherlands based customers. They are now working closely with the UK CAA and hope to receive approval later this week.
EMEA Senior Manager Maintenance Lee James, explained: �The development, approval and introduction of a new piece of equipment would usually take many months. We have achieved this � from first idea to implementation in daily flight routine � in two weeks.�
https://www.heliopsmag.com/chc-based...der-for-aw139A team of CHC engineers, based in Den Helder, Netherlands, has developed and fitted a plastic flexible cockpit/cabin divider that can be fitted to their AW139 fleet.
Highlighting real team work and collaboration between their technical services, maintenance, type technical pilots and management the system has been approved by, Leonardo Helicopters, the CAA-NL and Netherlands based customers. They are now working closely with the UK CAA and hope to receive approval later this week.
EMEA Senior Manager Maintenance Lee James, explained: �The development, approval and introduction of a new piece of equipment would usually take many months. We have achieved this � from first idea to implementation in daily flight routine � in two weeks.�

Join Date: Jul 2008
Location: Poland
Posts: 66
Likes: 0
Received 0 Likes
on
0 Posts
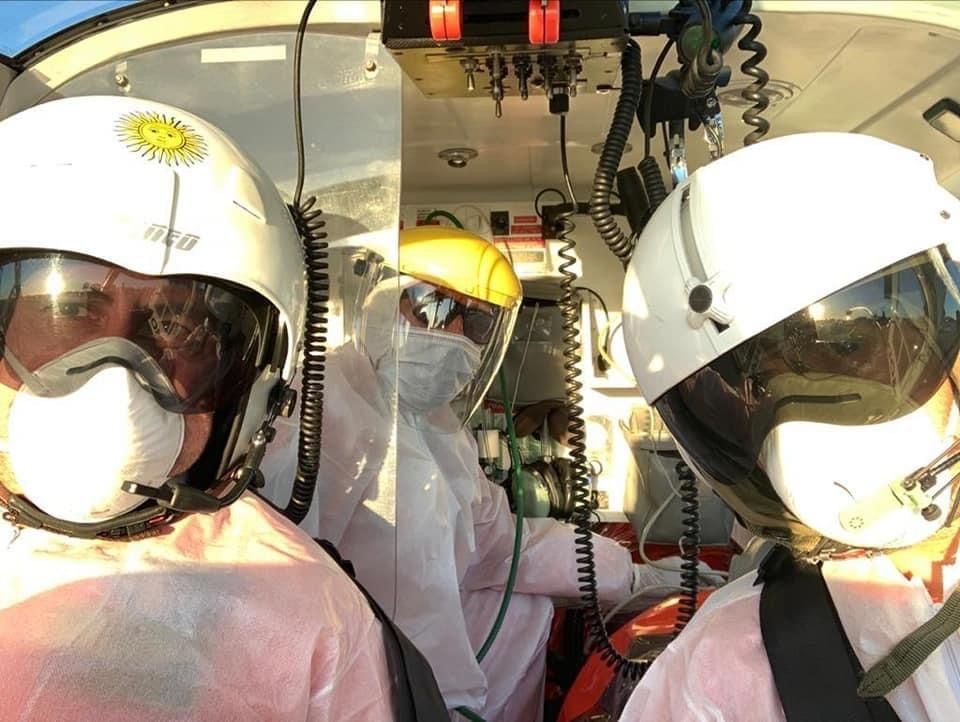
Argentina Modena
Here�s what Argentine HEMs operator Modena is using for its BO105 crews.
cheers





cheers
I am really posting to help those pilots doing this work as opposed to those just interested
The Italian photos show the use of FFP2 masks for the medical crew which do not protect them from AFPs. Not sure if the pilot's mask is FFP2 or FFP3 but unless you are actually joining in the intubation or lifting / moving the stretcher from the patient's head end an FFP2 meets the current guidelines.
The face shields are fine, but no better than a helmet with visor so I would just disconnect and leave my helmet on - changing from helmet to shield and back again is high risk. You cant do it without TWO hand cleans plus change of gloves plus container for helmet and shield and ideally a face and neck wash!! With a patient in the cab!!
The plastic coveralls again are questionable - flying overalls are as good. Just wash them. But my main gripe is the pilot has no gloves on and is touching his coveralls.
Unless you are transferring covid19 patients (and I see absolutely no indication) the patient is low risk. The risk is from the close proximity to ground crew, ops and especially the medical crew who may have been on a Covid 19 ward the day before!!!! Stay away from them. You can only get infected if the virus in their sputum gets into your airway. So masks for them and you at all times, wear gloves, and consider everything you touch to be contaminated so dont touch your face with your hands / gloves. The best way to achieve this is to keep your helmet on and visor down from walking out to changing at the end of shift and get someone to give you a lesson in donning and doffing or look online
As for the cabin isolation engineering, that only works if NOBODY in the front ever mixes with ANYONE in the back between proper cabin cleans at base. No paramedic in the front left seat. No pilot touching the stretcher, carrying cases or oxygen or helping with loading......Why not just stay in the cab, keep the front left seat empty and save your money
The Italian photos show the use of FFP2 masks for the medical crew which do not protect them from AFPs. Not sure if the pilot's mask is FFP2 or FFP3 but unless you are actually joining in the intubation or lifting / moving the stretcher from the patient's head end an FFP2 meets the current guidelines.
The face shields are fine, but no better than a helmet with visor so I would just disconnect and leave my helmet on - changing from helmet to shield and back again is high risk. You cant do it without TWO hand cleans plus change of gloves plus container for helmet and shield and ideally a face and neck wash!! With a patient in the cab!!
The plastic coveralls again are questionable - flying overalls are as good. Just wash them. But my main gripe is the pilot has no gloves on and is touching his coveralls.
Unless you are transferring covid19 patients (and I see absolutely no indication) the patient is low risk. The risk is from the close proximity to ground crew, ops and especially the medical crew who may have been on a Covid 19 ward the day before!!!! Stay away from them. You can only get infected if the virus in their sputum gets into your airway. So masks for them and you at all times, wear gloves, and consider everything you touch to be contaminated so dont touch your face with your hands / gloves. The best way to achieve this is to keep your helmet on and visor down from walking out to changing at the end of shift and get someone to give you a lesson in donning and doffing or look online
As for the cabin isolation engineering, that only works if NOBODY in the front ever mixes with ANYONE in the back between proper cabin cleans at base. No paramedic in the front left seat. No pilot touching the stretcher, carrying cases or oxygen or helping with loading......Why not just stay in the cab, keep the front left seat empty and save your money
As for the cabin isolation engineering, that only works if NOBODY in the front ever mixes with ANYONE in the back between proper cabin cleans at base. No paramedic in the front left seat. No pilot touching the stretcher, carrying cases or oxygen or helping with loading......Why not just stay in the cab, keep the front left seat empty and save your money
Exactly Fostex - that is why I was sceptical about cabin separation.
We also agree about transmission. I was pointing out the only way to get infected was to get virus from an infected person's airway into yours. There are indeed three ways this can happen:
Droplet from coughs and sneezes. A FFP2 mask on both the patient and recipient aims to stop this
Aerosol, mostly from intubation. A FFP3 mask is needed
Virus in sputum surviving as a fomite on surfaces and then being picked up on hands and transferred to the mouth. Gloves and not touching your face prevents this.
Glad of the opportunity to clarify. We need to give our colleagues clear advice and information. If anyone wants to PPM me please do and I will try my best to advise
Stay safe
We also agree about transmission. I was pointing out the only way to get infected was to get virus from an infected person's airway into yours. There are indeed three ways this can happen:
Droplet from coughs and sneezes. A FFP2 mask on both the patient and recipient aims to stop this
Aerosol, mostly from intubation. A FFP3 mask is needed
Virus in sputum surviving as a fomite on surfaces and then being picked up on hands and transferred to the mouth. Gloves and not touching your face prevents this.
Glad of the opportunity to clarify. We need to give our colleagues clear advice and information. If anyone wants to PPM me please do and I will try my best to advise
Stay safe
Does anyone know what is happening in the U.K. with regards to front seat crew PPE? There seems to be quite a few variations on a theme.
I ask as the company I work for are working hard to get a local solution for U.K. based Alpha helmet wearers and hope to have a stop gap half face respirator available, prior to the long term Gentex solution making its appearance (LPPR).
For anyone with experience of flying in FFP3 face masks, does the boom mic work effectively while wearing face masks or would a mask mounted mic be preferable/essential?
Opinions on wether a helmet mounted respirator solution would be better (put on/take off like an oxygen mask using side mounted connectors) than a completely separate
over the head face hugger type would also be welcome.
Best regards to those doing the biz during these times.
I ask as the company I work for are working hard to get a local solution for U.K. based Alpha helmet wearers and hope to have a stop gap half face respirator available, prior to the long term Gentex solution making its appearance (LPPR).
For anyone with experience of flying in FFP3 face masks, does the boom mic work effectively while wearing face masks or would a mask mounted mic be preferable/essential?
Opinions on wether a helmet mounted respirator solution would be better (put on/take off like an oxygen mask using side mounted connectors) than a completely separate
over the head face hugger type would also be welcome.
Best regards to those doing the biz during these times.
A single use FFP3 mask must be a complete seal so you have to be FIT tested using a hood and aerosols or there is a computer FIT test. If you arent FIT test it may be useless. A single use FFP3 mask must not be deformed so you cant push the mic into it. It only works for about 4 hours - written on the box - and provided it isnt wet.
Reusable FFP3 masks can be self tested because you can check you can create a vacuum. They are more comfortable. The filters last for weeks. The filters on the 7000 series from 3M are in a plastic casing and weather proof. BUT you must make sure the filter is classified as P3 - there are 7 different types of filter and P3 are in short supply. Using any other filter gives no protection...(a P2 will give the same as an ordinary surgical mask)
I have limited experience with a helmet mounted mask but I found it didnt provide a complete seal so useless for providing a viral barrier
The 3M 7000 series would be easy to mount a mic on the inside before sealing the plastic with sealant. I can easily make myself understood without shouting so an external boom mic may be OK and it doesnt matter of it touches the mask, but if anyone has used one with a standard mic I would be interested to hear.
Reusable FFP3 masks can be self tested because you can check you can create a vacuum. They are more comfortable. The filters last for weeks. The filters on the 7000 series from 3M are in a plastic casing and weather proof. BUT you must make sure the filter is classified as P3 - there are 7 different types of filter and P3 are in short supply. Using any other filter gives no protection...(a P2 will give the same as an ordinary surgical mask)
I have limited experience with a helmet mounted mask but I found it didnt provide a complete seal so useless for providing a viral barrier
The 3M 7000 series would be easy to mount a mic on the inside before sealing the plastic with sealant. I can easily make myself understood without shouting so an external boom mic may be OK and it doesnt matter of it touches the mask, but if anyone has used one with a standard mic I would be interested to hear.
Here some EHA information notice => the best practices applied by our members in the various EU Countries.
http://www.eha-heli.eu/images/News/I...NAL_090420.pdf
Regarding the mic and mask, some solution here -> https://www.heliopsmag.com/tiger-per...r-aviation-use
Also => look for some existing throat mic solutions from Kenwood, Motorola and similar, with price level 30 USD and up,
your local avionic shop can easy adapt one.
http://www.eha-heli.eu/images/News/I...NAL_090420.pdf
Regarding the mic and mask, some solution here -> https://www.heliopsmag.com/tiger-per...r-aviation-use
Also => look for some existing throat mic solutions from Kenwood, Motorola and similar, with price level 30 USD and up,
your local avionic shop can easy adapt one.
Good points. Just one thing I would add:
The virus is pathetic. It is easily destroyed by soap and water or detergent or indeed almost any cleaning fluid. The instruction to wash your hands for 20 seconds or whatever is to ensure all parts of the hands are washed - you dont need to keep the cleaner in contact for 20 seconds or immerse items unless it is the easiest thing to do. There is a concern less surfaces will be cleaned less frequently due to being over zealous or running out of 'approved' agents. I normally walk around with a disposable disinfectant cloth so that my gloves are continually being re soaked in the cleaner and so every door handle I touch is also touched by the cleaner....Maintenance rags soaked in washing up liquid or soapy water are probably just as good and hold their liquid much longer
The virus is pathetic. It is easily destroyed by soap and water or detergent or indeed almost any cleaning fluid. The instruction to wash your hands for 20 seconds or whatever is to ensure all parts of the hands are washed - you dont need to keep the cleaner in contact for 20 seconds or immerse items unless it is the easiest thing to do. There is a concern less surfaces will be cleaned less frequently due to being over zealous or running out of 'approved' agents. I normally walk around with a disposable disinfectant cloth so that my gloves are continually being re soaked in the cleaner and so every door handle I touch is also touched by the cleaner....Maintenance rags soaked in washing up liquid or soapy water are probably just as good and hold their liquid much longer
Join Date: Jun 2017
Location: Canada
Posts: 13
Likes: 0
Received 0 Likes
on
0 Posts
You are not a smart person. I'm sure you think you are, but that's just the Dunning-Kruger Effect
Join Date: Feb 2006
Location: Hanging off the end of a thread
Posts: 33,056
Received 2,927 Likes
on
1,250 Posts
EGNX today



Join Date: May 2007
Location: The Planet Earth
Age: 41
Posts: 24
Likes: 0
Received 0 Likes
on
0 Posts
Throat Mic's
Here some EHA information notice => the best practices applied by our members in the various EU Countries.
http://www.eha-heli.eu/images/News/I...NAL_090420.pdf
Regarding the mic and mask, some solution here -> https://www.heliopsmag.com/tiger-per...r-aviation-use
Also => look for some existing throat mic solutions from Kenwood, Motorola and similar, with price level 30 USD and up,
your local avionic shop can easy adapt one.
http://www.eha-heli.eu/images/News/I...NAL_090420.pdf
Regarding the mic and mask, some solution here -> https://www.heliopsmag.com/tiger-per...r-aviation-use
Also => look for some existing throat mic solutions from Kenwood, Motorola and similar, with price level 30 USD and up,
your local avionic shop can easy adapt one.
https://iasus-concepts.com/


