


What’s CASA doing with our sensitive medical information?

Thread Starter
What’s CASA doing with our sensitive medical information?
Among the most sensitive – if not the most sensitive – information about us is our medical information. Each time we make an application to CASA Avmed for a medical certificate, we provide them yet more sensitive information.
Because of my concern for aviation safety in the real world, where Avmed’s increasingly overreaching behaviour is resulting in pilots being increasingly unwilling to disclose information to Avmed and – worse still – to seek medical advice on potential issues for fear that it will get back to Avmed – an outcome inimical to aviation safety - I entered into some correspondence with CASA’s privacy folk recently. My correspondence was precipitated by my recollection that, years ago, there was a ‘tick box’, on the medical certificate application form, which you could tick to consent to the information in the form being used in medical studies. That tick box has gone. These days we’re apparently simply “acknowledging” that our information – “deidentified” – can be used in “research” (and “internal audit”).
(This is one of the many reasons for my description of us medical certificate applicants as “guinea pigs”. Each time we’re sent off to some expensive and sometimes risky tests which qualified specialists say are not justified, it appears we’re providing more data to Avmed for “research”. My educated guess is that the results of the “research” are used to justify Avmed’s own existence and the ‘need’ to intrude into the ‘management’ of the ever-increasing number of ‘aero-medically relevant’ conditions they keep discovering. I anticipate the results are also the subject of Avmed conference echo chambers.)
For my part, I disclose my information for the purpose of, and only for the purpose of, being assessed against the statutory criteria for the issue of a medical certificate. I either meet those criteria or I don’t, and whether my information – deidentified or otherwise – is used in research is irrelevant to that question.
In essence, I asked how CASA got the job of using or disclosing our deidentified sensitive medical information for “research” purposes. I noted that the word “research” appears nowhere in CASA’s functions in the Civil Aviation Act. (CASA does have the function of, for example, cooperating with the Australian Transport Safety Bureau in relation to investigations under the TSI Act that relate to aircraft, and the ATSB can compel CASA to provide medical information about us in the course an investigation. There’s no deidentification required in that case, for obvious reasons.) CASA doesn’t have the corporate competence to do the jobs that are actually stated in the Civil Aviation Act – among the elephants in that room is “developing … concise aviation safety standards” – so better to focus on those than chasing medical research butterflies.
In essence, the CASA person’s response is that CASA has the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not.
I have raised this issue, among related issues, with the Office of the Australian Information Commissioner (OAIC).
Assuming CASA does have the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not, it raises the question as to effectiveness of the procedures used in fact by CASA to achieve deidentification. (The OAIC has much to say on deidentification.) Given my first-hand experience in AAT matters against CASA and the content of CASA documents, disclosed under FOI, about how Avmed conducts itself, I have little faith in the effectiveness of whatever little governance arrangements are placed around Avmed’s activities.
I have submitted FOI requests to CASA in the following terms on Friday (18 Aug 2023):
I will keep everyone informed of the OAIC’s response and the outcomes of my FOI requests.
Because of my concern for aviation safety in the real world, where Avmed’s increasingly overreaching behaviour is resulting in pilots being increasingly unwilling to disclose information to Avmed and – worse still – to seek medical advice on potential issues for fear that it will get back to Avmed – an outcome inimical to aviation safety - I entered into some correspondence with CASA’s privacy folk recently. My correspondence was precipitated by my recollection that, years ago, there was a ‘tick box’, on the medical certificate application form, which you could tick to consent to the information in the form being used in medical studies. That tick box has gone. These days we’re apparently simply “acknowledging” that our information – “deidentified” – can be used in “research” (and “internal audit”).
(This is one of the many reasons for my description of us medical certificate applicants as “guinea pigs”. Each time we’re sent off to some expensive and sometimes risky tests which qualified specialists say are not justified, it appears we’re providing more data to Avmed for “research”. My educated guess is that the results of the “research” are used to justify Avmed’s own existence and the ‘need’ to intrude into the ‘management’ of the ever-increasing number of ‘aero-medically relevant’ conditions they keep discovering. I anticipate the results are also the subject of Avmed conference echo chambers.)
For my part, I disclose my information for the purpose of, and only for the purpose of, being assessed against the statutory criteria for the issue of a medical certificate. I either meet those criteria or I don’t, and whether my information – deidentified or otherwise – is used in research is irrelevant to that question.
In essence, I asked how CASA got the job of using or disclosing our deidentified sensitive medical information for “research” purposes. I noted that the word “research” appears nowhere in CASA’s functions in the Civil Aviation Act. (CASA does have the function of, for example, cooperating with the Australian Transport Safety Bureau in relation to investigations under the TSI Act that relate to aircraft, and the ATSB can compel CASA to provide medical information about us in the course an investigation. There’s no deidentification required in that case, for obvious reasons.) CASA doesn’t have the corporate competence to do the jobs that are actually stated in the Civil Aviation Act – among the elephants in that room is “developing … concise aviation safety standards” – so better to focus on those than chasing medical research butterflies.
In essence, the CASA person’s response is that CASA has the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not.
I have raised this issue, among related issues, with the Office of the Australian Information Commissioner (OAIC).
Assuming CASA does have the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not, it raises the question as to effectiveness of the procedures used in fact by CASA to achieve deidentification. (The OAIC has much to say on deidentification.) Given my first-hand experience in AAT matters against CASA and the content of CASA documents, disclosed under FOI, about how Avmed conducts itself, I have little faith in the effectiveness of whatever little governance arrangements are placed around Avmed’s activities.
I have submitted FOI requests to CASA in the following terms on Friday (18 Aug 2023):
All documents containing current CASA policy on and procedures for deidentification of originally sensitive medical information supplied by applicants for medical certificates, prior to disclosure or use by CASA for the purposes of research.
All documents containing information about the assessment of the effectiveness of CASA’s deidentification procedures, including the application of the ‘motivated intruder’ test, to mitigate the risks of reidentification of the individuals to whom the originally sensitive medical information relates.
All documents containing information about results of audits, conducted by auditors internal or external to CASA, of CASA’s compliance with CASA policy on and procedures for deidentification of originally sensitive medical information.
All documents containing information about the disclosure or use by CASA of deidentified originally sensitive medical information supplied by applicants for medical certificates, if the information in the documents includes any one or more or all of the following: The purpose of the disclosure or use of the deidentified information; the identity of the persons – natural or otherwise – to whom the deidentified information was disclosed; any description of the disclosed deidentified information; the results of the use to which the disclosed deidentified information was put.
All documents containing information about the assessment of the effectiveness of CASA’s deidentification procedures, including the application of the ‘motivated intruder’ test, to mitigate the risks of reidentification of the individuals to whom the originally sensitive medical information relates.
All documents containing information about results of audits, conducted by auditors internal or external to CASA, of CASA’s compliance with CASA policy on and procedures for deidentification of originally sensitive medical information.
All documents containing information about the disclosure or use by CASA of deidentified originally sensitive medical information supplied by applicants for medical certificates, if the information in the documents includes any one or more or all of the following: The purpose of the disclosure or use of the deidentified information; the identity of the persons – natural or otherwise – to whom the deidentified information was disclosed; any description of the disclosed deidentified information; the results of the use to which the disclosed deidentified information was put.

The following 3 users liked this post by Clinton McKenzie:
AVMAD
Many thanks Clinton McKenzie for raising and acting upon an important issue. I completely agree with the points made, myself having had to repeatedly undertake medical tests by AVMED against specialist advice and which tests my DAME believes are unnecessary. The latter gentleman having been in practice for at least some 40 years, and pilot to boot.
But time money and real life outcomes mean absolutely nothing to AVMED, as instanced by CASA’s answer to the highly successful BasicMed reform in the USA.
Our version, the Basic Class 2 (BC2), is a perversion.
It could have been very useful had CASA followed the USA model. But of course no, our model is ‘better’ because it’s far more stringent and doesn’t allow IFR. Well naturally you wouldn’t want to encourage people to fly around when they can’t see out the windows would you? Surely that’s not safe.
But wait, there’s more, and wait, and wait, presently CASA is looking again at a new self declared type medical certification. Interminable discussions are proceeding at a sluggish snails pace to further this possible reform when with stroke of pen the current BC2 could have the car driver standard instead of ‘unconditional commercial heavy vehicle’ and even allowed IFR. ‘Conditional’ fuel tanker drivers are on our roads everywhere but flying your Cessna around at that standard is way to risky for CASA. Meanwhile there are droves of pilots giving up on AVMED and either leaving the field entirely or taking up flying with RAAUS. Several thousand of that cohort not doing aviation medicals at all, no problem the last 40 years.
Truth is CASA has no incentives to simplify or create clear and concise rules or practices because that would result in less ‘work.’ It’s disgraceful that we’ve not had a Board or CEO with the fortitude of character to correct the numerous failings of CASA or recognise that aviation has taken a battering for no good reason.
In the absence of political leadership, in particular stuck as we are with a wrong model of governance, should be a Department with responsible Minister (it’s called Westminster democracy), we must hold to account CASA itself to see the huge opportunities for services and job creation if only rational policies are enacted.
But time money and real life outcomes mean absolutely nothing to AVMED, as instanced by CASA’s answer to the highly successful BasicMed reform in the USA.
Our version, the Basic Class 2 (BC2), is a perversion.
It could have been very useful had CASA followed the USA model. But of course no, our model is ‘better’ because it’s far more stringent and doesn’t allow IFR. Well naturally you wouldn’t want to encourage people to fly around when they can’t see out the windows would you? Surely that’s not safe.
But wait, there’s more, and wait, and wait, presently CASA is looking again at a new self declared type medical certification. Interminable discussions are proceeding at a sluggish snails pace to further this possible reform when with stroke of pen the current BC2 could have the car driver standard instead of ‘unconditional commercial heavy vehicle’ and even allowed IFR. ‘Conditional’ fuel tanker drivers are on our roads everywhere but flying your Cessna around at that standard is way to risky for CASA. Meanwhile there are droves of pilots giving up on AVMED and either leaving the field entirely or taking up flying with RAAUS. Several thousand of that cohort not doing aviation medicals at all, no problem the last 40 years.
Truth is CASA has no incentives to simplify or create clear and concise rules or practices because that would result in less ‘work.’ It’s disgraceful that we’ve not had a Board or CEO with the fortitude of character to correct the numerous failings of CASA or recognise that aviation has taken a battering for no good reason.
In the absence of political leadership, in particular stuck as we are with a wrong model of governance, should be a Department with responsible Minister (it’s called Westminster democracy), we must hold to account CASA itself to see the huge opportunities for services and job creation if only rational policies are enacted.
The following 3 users liked this post by Sandy Reith:
Thread Starter
Unfortunately, there is insufficient governance around Avmed, Sandy.
There is an interesting, relatively-recent decision of the AAT which highlights, again, all which is wrong in Avmed and why it has become a force inimical to aviation safety. Fortunately the Deputy President in the matter saw through Avmed’s usual smoke and mirrors created by the shibboleth of the safety of air navigation.
As background to the insufficient governance point, I note an AAT matter challenging a decision of erstwhile PMO, Pooshan Navathe, from 2013 in which the Tribunal said:
The Tribunal’s trust was misplaced.
One recent example of CASA once again trying to trot out the Avmed decision-maker to give evidence as to why their decision was the correct and preferable one is Bush and Civil Aviation Safety Authority [2022] AATA 2821 (26 August 2022), in which the Tribunal said:
Sounds very familiar, doesn’t it. And CASA has tried the same trick in other matters post-Bolton, despite what it was told in Bolton.
Having been sent an unequivocal message from the Tribunal in Bolton – which message the Tribunal should not have had to send in the first place - that the Avmed decision-maker is not truly independent and, therefore, is not qualified to give expert opinion on the substance of the decision in question, CASA ignored the Tribunal. CASA continued, and continues, to trot out Avmed people to advocate for their own decisions because – well – they know best.
Of course the decision-maker’s decision is the correct and preferable one. Just ask them. Everything CASA does is reasonable and appropriate. Just ask them.
Avmed’s modus operandi is to do whatever it likes, comfortable in the belief that few victims can handle the cost and stress of taking them to external review and, in the few cases in which they are taken on, Avmed will scaremonger its way into eventually convincing the Tribunal to accept some plausible approach or opinion put to it, which CASA then seizes on as a precedent for future Tribunal matters. (I use the word “plausible” in its correct sense: “superficially fair, reasonable, or valuable but often specious”.) If the Tribunal accepts some approach or opinion put to it by Avmed, that’s treated as precedent by Avmed. If the Tribunal tells Avmed something it doesn’t want to hear – like they’re not qualified to give expert opinion evidence about the substance of their own decisions - that’s an inconvenience to be ignored. Avmed just tries it again, at the next opportunity.
If there were any proper governance around them, Navathe wouldn’t have been allowed by CASA to advocate for his own decision in Bolton in the first place. Nor would Navathe have been allowed to do the other appalling thing which was identified by the Tribunal in that matter:
It is not known what documentary material was provided to Dr Somerville nor is it known what was conveyed to him by Dr Navathe in the conversation on 1 November 2013. Moreover, it is highly irregular that one expert witness, who is as well the primary decision-maker, was apparently briefing another expert witness in terms not disclosed. The danger of such a practice ought to have been evident. The vice is merely compounded by the failure to make clear what information was conveyed.
Nor would Dr Beresford have been allowed to put in a statement to the Tribunal in the Bush matter, to the extent the statement contained her opinions about the substance of her decision under review.
These are public officials being allowed to do things which they and CASA have been told, time-and time-again, not to do. And they’re doing it with the assistance of CASA lawyers who then try to defend it in the Tribunal. This is a manifestation of an organisation with insufficient corporate competence and insufficient corporate integrity. Plain and simple.
I’m not suggesting the people involved are dishonest. This isn’t a matter of people lying. This is a matter of people either not understanding their duties as public officials or understanding them but choosing to ignore them.
As to other plausible approaches and opinions tried on by Avmed, it was relieving to see that the Tribunal in the Bush matter saw through the mystique of aviation that has been used to bamboozle so often in the past:
That last paragraph is a merciful voice of reason.
But bear in mind who writes the ICAO “Manual of Civil Aviation Medicine”. What would be the purposes of the “research” for which CASA uses or discloses our medical information? Would its results ever likely be construed as suggesting that Avmed’s behaviours are a harmful overreaction to the objective risks? Methinks not. Methinks the results go into an echo chamber of Avmed people justifying their existence.
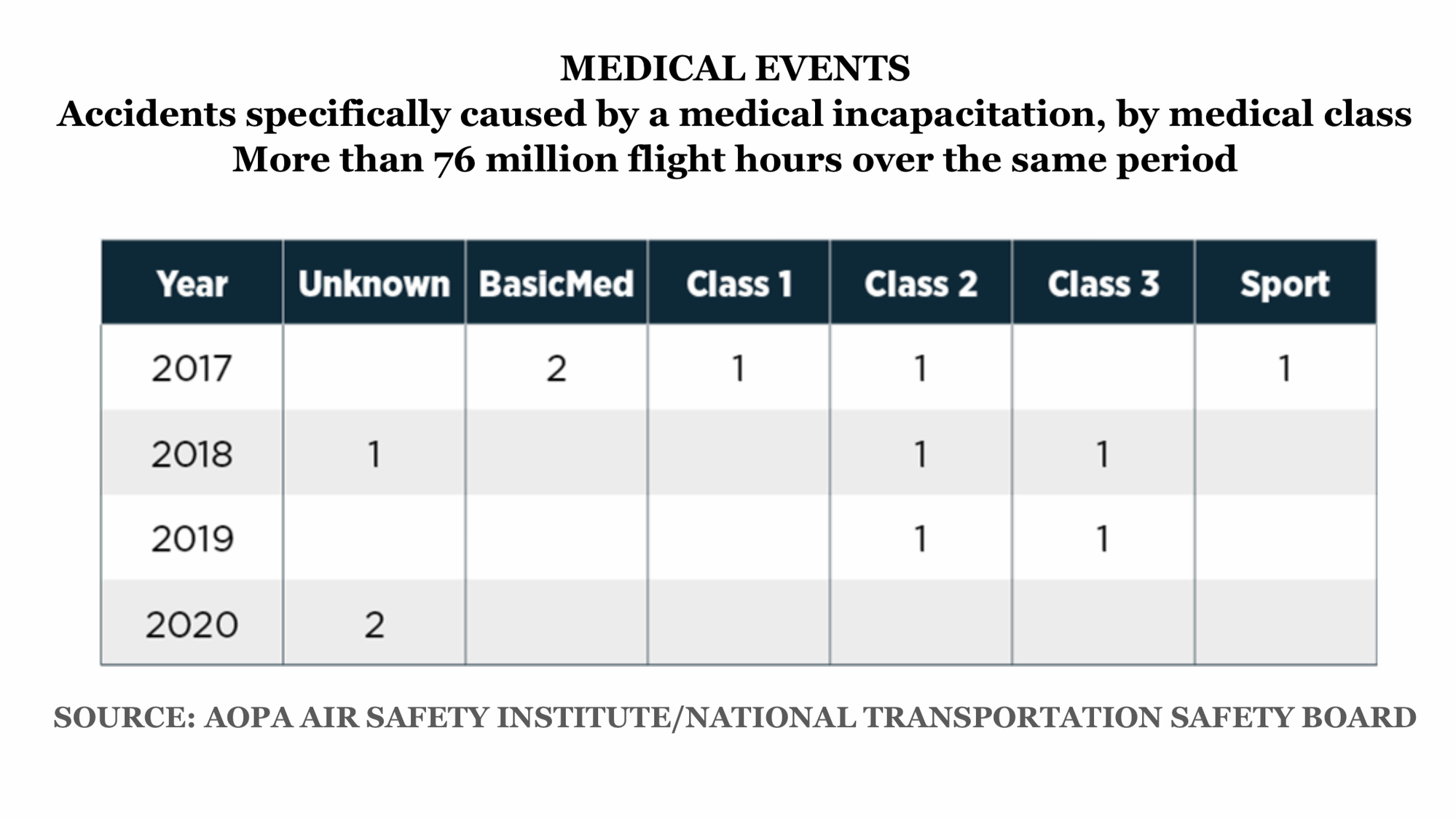
These already-available research results, conducted by people without a conflict of interest, suggest Avmed’s doing some harm to aviation safety:
Medical bureaucrats are the last people who should have any involvement in that work.
(The good news is that in Bush - as with many challenges to CASA Avmed decisions in the last 15 or so years – Avmed’s decision was set aside and Bush was issued with a Class 2 medical certificate. There were some conditions imposed to deal with the awful risks to the safety of air navigation pressed by CASA. Presumably the information provided by Bush in compliance with those conditions will be used or disclosed by CASA for the purposes of “research”.)
There is an interesting, relatively-recent decision of the AAT which highlights, again, all which is wrong in Avmed and why it has become a force inimical to aviation safety. Fortunately the Deputy President in the matter saw through Avmed’s usual smoke and mirrors created by the shibboleth of the safety of air navigation.
As background to the insufficient governance point, I note an AAT matter challenging a decision of erstwhile PMO, Pooshan Navathe, from 2013 in which the Tribunal said:
Despite the fact that [Navathe’s] statement does contain the declaration of duty required by the Guidelines [for Persons Giving Expert and Opinion Evidence] it could not be plainer that Dr Navathe is an advocate for his own decision. I do not propose to have any regard to his opinions. For the future I would trust that CASA’s Legal Branch would exercise independent judgement in deciding what witnesses ought be relied upon and the content of their statements. They ought, obviously enough, be confined to matters that are relevant and witnesses ought be those who can truly provide an independent opinion.
One recent example of CASA once again trying to trot out the Avmed decision-maker to give evidence as to why their decision was the correct and preferable one is Bush and Civil Aviation Safety Authority [2022] AATA 2821 (26 August 2022), in which the Tribunal said:
Dr Beresford, then, went [on in her statement] to deal with whether the Applicant met the Class 2 Medical Standard. This part of her statement is not helpful, as Dr Beresford, again, explains why she reached her conclusion in the reviewable decision. For the reasons outlined above, the Tribunal does not place any weight on this part of the statement.
Having been sent an unequivocal message from the Tribunal in Bolton – which message the Tribunal should not have had to send in the first place - that the Avmed decision-maker is not truly independent and, therefore, is not qualified to give expert opinion on the substance of the decision in question, CASA ignored the Tribunal. CASA continued, and continues, to trot out Avmed people to advocate for their own decisions because – well – they know best.
Of course the decision-maker’s decision is the correct and preferable one. Just ask them. Everything CASA does is reasonable and appropriate. Just ask them.
Avmed’s modus operandi is to do whatever it likes, comfortable in the belief that few victims can handle the cost and stress of taking them to external review and, in the few cases in which they are taken on, Avmed will scaremonger its way into eventually convincing the Tribunal to accept some plausible approach or opinion put to it, which CASA then seizes on as a precedent for future Tribunal matters. (I use the word “plausible” in its correct sense: “superficially fair, reasonable, or valuable but often specious”.) If the Tribunal accepts some approach or opinion put to it by Avmed, that’s treated as precedent by Avmed. If the Tribunal tells Avmed something it doesn’t want to hear – like they’re not qualified to give expert opinion evidence about the substance of their own decisions - that’s an inconvenience to be ignored. Avmed just tries it again, at the next opportunity.
If there were any proper governance around them, Navathe wouldn’t have been allowed by CASA to advocate for his own decision in Bolton in the first place. Nor would Navathe have been allowed to do the other appalling thing which was identified by the Tribunal in that matter:
Finally, CASA relied upon evidence (including a report of 4 November 2013) of Dr Ernest Somerville, a consultant neurologist. I have already made mention of the reference in Dr Somerville's report to a document from the Proserpine Hospital which is not in evidence in the proceedings. The failure to comply with the Guidelines is exemplified by this passage from Dr Somerville's report:
The following opinion is provided in response to your letter of 30 October 2013 and telephone conversation with Dr Pooshan Navathe on 1 November 2013. Information about Mr Walker's [sic] medical condition is limited to the documents provided with your letter of 30 October 2013.
It is not known what documentary material was provided to Dr Somerville nor is it known what was conveyed to him by Dr Navathe in the conversation on 1 November 2013. Moreover, it is highly irregular that one expert witness, who is as well the primary decision-maker, was apparently briefing another expert witness in terms not disclosed. The danger of such a practice ought to have been evident. The vice is merely compounded by the failure to make clear what information was conveyed.
These are public officials being allowed to do things which they and CASA have been told, time-and time-again, not to do. And they’re doing it with the assistance of CASA lawyers who then try to defend it in the Tribunal. This is a manifestation of an organisation with insufficient corporate competence and insufficient corporate integrity. Plain and simple.
I’m not suggesting the people involved are dishonest. This isn’t a matter of people lying. This is a matter of people either not understanding their duties as public officials or understanding them but choosing to ignore them.
As to other plausible approaches and opinions tried on by Avmed, it was relieving to see that the Tribunal in the Bush matter saw through the mystique of aviation that has been used to bamboozle so often in the past:
The Tribunal was presented with some evidence about the annualised risk of incapacitation. In particular, reference was made to the 1% and 2% rule. It needs to be emphasised, at the outset, that neither the Act nor the Regulations prescribe such a rule. As was emphasised in Mulholland, and which is accepted by the Tribunal, the task of the decision-maker is to determine what is likely to endanger the safety of air navigation.
Having noted this important starting point, the Tribunal also accepts, as noted in Collins and Civil Aviation Safety Authority [2017] AATA 2564 (Collins), that “the internationally accepted guideline can play a useful, if not critical, exercise in assessing risk and in ensuring consistency in decision making concerning air navigation safety” – at [76].
The 1% rule is set out and explained in the International Civil Aviation Organisation Manual of Civil Aviation Medicine. This Organisation is a United Nations agency established in 1944 which governs the Convention on International Civil Aviation (the Chicago Convention), of which, Australia is a Member State.
Further, pursuant to s 11 of the Act, CASA must perform its functions in a manner consistent with the obligations of the Commonwealth under the Chicago Convention.
As noted in Collins (at [74]), CASA allows for a 2% annualised risk of incapacitation for Class 2 medical certificates because of the different profile of flying, namely, private and non-commercial.
In short, neither the 1% nor 2% rule have their foundations in a specific provision in either the Act or Regulations. However, pursuant to Article 37 of the Chicago Convention which requires Member States to collaborate in securing the highest degree of uniformity in regulations, standards and procedures, the 1% rule should be regarded as a sound starting point or guide when measuring risk.
However, as will be discussed below, the measurement of risk is not, of itself, a purely arithmetic and clinically objective task. It may be that, with common ailments that afflict many members of the community, learned research has been undertaken that would allow the calculation of potential risk with a high degree of precision. In comparison, there are other ailments that are rare, and the condition afflicting persons varies, and is sometimes, idiosyncratic. In such cases, the development of an annualised risk assessment of incapacitation, becomes more problematic and less precise.
Having noted this important starting point, the Tribunal also accepts, as noted in Collins and Civil Aviation Safety Authority [2017] AATA 2564 (Collins), that “the internationally accepted guideline can play a useful, if not critical, exercise in assessing risk and in ensuring consistency in decision making concerning air navigation safety” – at [76].
The 1% rule is set out and explained in the International Civil Aviation Organisation Manual of Civil Aviation Medicine. This Organisation is a United Nations agency established in 1944 which governs the Convention on International Civil Aviation (the Chicago Convention), of which, Australia is a Member State.
Further, pursuant to s 11 of the Act, CASA must perform its functions in a manner consistent with the obligations of the Commonwealth under the Chicago Convention.
As noted in Collins (at [74]), CASA allows for a 2% annualised risk of incapacitation for Class 2 medical certificates because of the different profile of flying, namely, private and non-commercial.
In short, neither the 1% nor 2% rule have their foundations in a specific provision in either the Act or Regulations. However, pursuant to Article 37 of the Chicago Convention which requires Member States to collaborate in securing the highest degree of uniformity in regulations, standards and procedures, the 1% rule should be regarded as a sound starting point or guide when measuring risk.
However, as will be discussed below, the measurement of risk is not, of itself, a purely arithmetic and clinically objective task. It may be that, with common ailments that afflict many members of the community, learned research has been undertaken that would allow the calculation of potential risk with a high degree of precision. In comparison, there are other ailments that are rare, and the condition afflicting persons varies, and is sometimes, idiosyncratic. In such cases, the development of an annualised risk assessment of incapacitation, becomes more problematic and less precise.
But bear in mind who writes the ICAO “Manual of Civil Aviation Medicine”. What would be the purposes of the “research” for which CASA uses or discloses our medical information? Would its results ever likely be construed as suggesting that Avmed’s behaviours are a harmful overreaction to the objective risks? Methinks not. Methinks the results go into an echo chamber of Avmed people justifying their existence.
These already-available research results, conducted by people without a conflict of interest, suggest Avmed’s doing some harm to aviation safety:
Results: A total of 3765 pilots were included in the analysis. There were 56.1% of pilots (n = 2111) who reported a history of healthcare avoidance behavior due fear for losing their aeromedical certificate. There were 45.7% who sought informal medical care (n = 1721) and 26.8% who misrepresented/withheld information on a written healthcare questionnaire for fear of aeromedical certificate loss (n = 994).
Conclusions: Aircraft pilots may participate in healthcare avoidance behavior related to fear of losing their aeromedical certificate. Further work is necessary to address pilot healthcare avoidance.
Conclusions: Aircraft pilots may participate in healthcare avoidance behavior related to fear of losing their aeromedical certificate. Further work is necessary to address pilot healthcare avoidance.
(The good news is that in Bush - as with many challenges to CASA Avmed decisions in the last 15 or so years – Avmed’s decision was set aside and Bush was issued with a Class 2 medical certificate. There were some conditions imposed to deal with the awful risks to the safety of air navigation pressed by CASA. Presumably the information provided by Bush in compliance with those conditions will be used or disclosed by CASA for the purposes of “research”.)
AVMAD
Hats off to Clinton and Pilot Bush for choosing to take on CASA’s aviation branch.
Without root and branch reform, nothing will change the course of AVMED’s relentless attacks on individuals. AVMED will completely ignore appeals to reason such as the absence of a risk profile that might give credence to its otherwise destructive path.
The whole sorry saga also causes questions around the AAT system which in the first place was instigated to provide an informal low cost alternative to the regular courts. It was a huge mistake, you won’t find justice by throwing out the numerous hard learned lessons and principles that make up our British legal system. Governments should make our traditional courts far more accessible and provide assistance to those who need recourse against bureaucratic shenanigans.
Without root and branch reform, nothing will change the course of AVMED’s relentless attacks on individuals. AVMED will completely ignore appeals to reason such as the absence of a risk profile that might give credence to its otherwise destructive path.
The whole sorry saga also causes questions around the AAT system which in the first place was instigated to provide an informal low cost alternative to the regular courts. It was a huge mistake, you won’t find justice by throwing out the numerous hard learned lessons and principles that make up our British legal system. Governments should make our traditional courts far more accessible and provide assistance to those who need recourse against bureaucratic shenanigans.

Thread Starter
We'll have to agree to disagree on your argument that the AAT was a "mistake", Sandy. Many pilots' careers and life's passion have been saved by the AAT. "Traditional courts" don't do merits review.
The AAT isn't perfect - far from it. Under-resourcing doesn't help. Stacking it with political mates doesn't help. But the underlying concept is sound and has proven itself as such, more often than not.
In the mid-2000s the coalition government said it was going to abolish the AAT. Didn't happen. The current government said it was going to abolish the AAT. Won't happen (though maybe a name change will). The "traditional courts" would be completely overwhelmed if they were given jurisdiction for the matters currently considered by the AAT.
The AAT isn't perfect - far from it. Under-resourcing doesn't help. Stacking it with political mates doesn't help. But the underlying concept is sound and has proven itself as such, more often than not.
In the mid-2000s the coalition government said it was going to abolish the AAT. Didn't happen. The current government said it was going to abolish the AAT. Won't happen (though maybe a name change will). The "traditional courts" would be completely overwhelmed if they were given jurisdiction for the matters currently considered by the AAT.
The following users liked this post:
Join Date: Apr 2008
Location: Australia
Posts: 490
Likes: 0
Received 0 Likes
on
0 Posts
reference was made to the 1% and 2% rule
Also, 1% and 2% of what? 1% seems way too high to be a figure for in flight incapacitation. I assume it must be incapacitation at any time during the year. In which case the standard for private pilots seems unreasonably high in relative terms.
A commercial pilot probably flies 10x the hours of the average private pilot, flies under commercial pressures, and many fly multiple passenger commercial operations single pilot. So the relative risk to the public from an incapacitated commercial pilot is much higher than the 1% vs 2% numbers allow for. If the standards are objectively based on risk, the commercial pilot standards should be many times higher than the private pilot, not just 50% reduction in risk.
Thread Starter
That's how Avmed 'justifies' its approach. "Curious" is one word for it. Track down someone with actuarial qualifications and run the statistical logic past them.
And some private pilots fly many more hours a year, with many more passengers, than some holders of a commercial licence.
The only pilots I know who've died while at the controls, suddenly, of undiagnosed conditions were the holders of ... Class 1 medical certificates.
And some private pilots fly many more hours a year, with many more passengers, than some holders of a commercial licence.
The only pilots I know who've died while at the controls, suddenly, of undiagnosed conditions were the holders of ... Class 1 medical certificates.
Join Date: Apr 2008
Location: Australia
Posts: 490
Likes: 0
Received 0 Likes
on
0 Posts
What do you mean justifies it's approach? It means they can't justify anything unless they can produce actual, achieved numbers. In particular, it means that for private pilots they need to show that the number is between 1% and 2%, or the standards they are applying are inappropriate.
Some private pilots... some commercial pilots... meaningless for risk assessment. If you are assessing risk you need to pick a meaningful benchmark - probably average passenger hours, but maybe you want e.g. 95th percentile of worst case. Worst case risk for commercial pilots is pretty bad - e.g, pilots doing hundreds of hours carrying paying passengers in whatever the largest aircraft is that can be flown single pilot.
Some private pilots... some commercial pilots... meaningless for risk assessment. If you are assessing risk you need to pick a meaningful benchmark - probably average passenger hours, but maybe you want e.g. 95th percentile of worst case. Worst case risk for commercial pilots is pretty bad - e.g, pilots doing hundreds of hours carrying paying passengers in whatever the largest aircraft is that can be flown single pilot.
Thread Starter
Don’t shoot me as the messenger. Ask Avmed. But don’t expect to be convinced by the substance of the response.
I am so glad that I don't need an Australian Medical anymore, because I fly foreign registered aircraft! F CASA AVMED!
Thread Starter
Update
As you will see from my original post, I submitted FOI requests to CASA in the following terms on 18 August 2023:
The responses:
So there you have it.
Another manifestation of governance failures in CASA and the carefree contempt of Avmed for us guinea pigs.
I'll inform the OAIC accordingly.
All documents containing current CASA policy on and procedures for deidentification of originally sensitive medical information supplied by applicants for medical certificates, prior to disclosure or use by CASA for the purposes of research.
All documents containing information about the assessment of the effectiveness of CASA’s deidentification procedures, including the application of the ‘motivated intruder’ test, to mitigate the risks of reidentification of the individuals to whom the originally sensitive medical information relates.
All documents containing information about results of audits, conducted by auditors internal or external to CASA, of CASA’s compliance with CASA policy on and procedures for deidentification of originally sensitive medical information.
All documents containing information about the disclosure or use by CASA of deidentified originally sensitive medical information supplied by applicants for medical certificates, if the information in the documents includes any one or more or all of the following: The purpose of the disclosure or use of the deidentified information; the identity of the persons – natural or otherwise – to whom the deidentified information was disclosed; any description of the disclosed deidentified information; the results of the use to which the disclosed deidentified information was put.
All documents containing information about the assessment of the effectiveness of CASA’s deidentification procedures, including the application of the ‘motivated intruder’ test, to mitigate the risks of reidentification of the individuals to whom the originally sensitive medical information relates.
All documents containing information about results of audits, conducted by auditors internal or external to CASA, of CASA’s compliance with CASA policy on and procedures for deidentification of originally sensitive medical information.
All documents containing information about the disclosure or use by CASA of deidentified originally sensitive medical information supplied by applicants for medical certificates, if the information in the documents includes any one or more or all of the following: The purpose of the disclosure or use of the deidentified information; the identity of the persons – natural or otherwise – to whom the deidentified information was disclosed; any description of the disclosed deidentified information; the results of the use to which the disclosed deidentified information was put.
I have conducted a thorough search of CASAs registry files and liaised with several CASA
business units in conducting this search, I was unable to locate any documents relevant to
the scope of your request[s].
business units in conducting this search, I was unable to locate any documents relevant to
the scope of your request[s].
Another manifestation of governance failures in CASA and the carefree contempt of Avmed for us guinea pigs.
I'll inform the OAIC accordingly.
The following users liked this post:
What’s it doing with medical info? And our tax dollars?
Table 1.1: CASA resource statement — Budget estimates for 2023-24 as at Budget May 2023
2022-23 Estimated actual
$'000
2023-24 Estimate
$'000
Opening balance/cash reserves at 1 July
82,473
79,698
Funds from Government
Annual appropriations - ordinary annual services(a)(b)
Outcome 1
91,155
107,602
Total annual appropriations
91,155
107,602
Special appropriations
Aviation Fuel Revenues (Special Appropriation) Act 1988
113,247
88,844
RPAS under s46A(4) of the Civil Aviation Act 1988
1,832
1,000
Total special appropriations
115,079
89,844
Total funds from Government
206,234
197,446
Funds from industry sources
Regulatory service fees
8,239
12,500
Total funds from industry sources
8,239
12,500
Funds from other sources
Interest
1,476
2,416
Other
318
886
Total funds from other sources
1,794
3,302
Total net resourcing for CASA
298,740
292,946
———————/—-/—————————-
Above copied from ‘infrastructure.gov.au’
Add the three zeros to that last figure and
this is the bottom line, the annual budget for CASA is $292,946,000
What do we get for $300 million?
The money is truly staggering, last time I looked it was $200 million.
2022-23 Estimated actual
$'000
2023-24 Estimate
$'000
Opening balance/cash reserves at 1 July
82,473
79,698
Funds from Government
Annual appropriations - ordinary annual services(a)(b)
Outcome 1
91,155
107,602
Total annual appropriations
91,155
107,602
Special appropriations
Aviation Fuel Revenues (Special Appropriation) Act 1988
113,247
88,844
RPAS under s46A(4) of the Civil Aviation Act 1988
1,832
1,000
Total special appropriations
115,079
89,844
Total funds from Government
206,234
197,446
Funds from industry sources
Regulatory service fees
8,239
12,500
Total funds from industry sources
8,239
12,500
Funds from other sources
Interest
1,476
2,416
Other
318
886
Total funds from other sources
1,794
3,302
Total net resourcing for CASA
298,740
292,946
———————/—-/—————————-
Above copied from ‘infrastructure.gov.au’
Add the three zeros to that last figure and
this is the bottom line, the annual budget for CASA is $292,946,000
What do we get for $300 million?
The money is truly staggering, last time I looked it was $200 million.
Among the most sensitive – if not the most sensitive – information about us is our medical information. Each time we make an application to CASA Avmed for a medical certificate, we provide them yet more sensitive information.
Because of my concern for aviation safety in the real world, where Avmed’s increasingly overreaching behaviour is resulting in pilots being increasingly unwilling to disclose information to Avmed and – worse still – to seek medical advice on potential issues for fear that it will get back to Avmed – an outcome inimical to aviation safety - I entered into some correspondence with CASA’s privacy folk recently. My correspondence was precipitated by my recollection that, years ago, there was a ‘tick box’, on the medical certificate application form, which you could tick to consent to the information in the form being used in medical studies. That tick box has gone. These days we’re apparently simply “acknowledging” that our information – “deidentified” – can be used in “research” (and “internal audit”).
(This is one of the many reasons for my description of us medical certificate applicants as “guinea pigs”. Each time we’re sent off to some expensive and sometimes risky tests which qualified specialists say are not justified, it appears we’re providing more data to Avmed for “research”. My educated guess is that the results of the “research” are used to justify Avmed’s own existence and the ‘need’ to intrude into the ‘management’ of the ever-increasing number of ‘aero-medically relevant’ conditions they keep discovering. I anticipate the results are also the subject of Avmed conference echo chambers.)
For my part, I disclose my information for the purpose of, and only for the purpose of, being assessed against the statutory criteria for the issue of a medical certificate. I either meet those criteria or I don’t, and whether my information – deidentified or otherwise – is used in research is irrelevant to that question.
In essence, I asked how CASA got the job of using or disclosing our deidentified sensitive medical information for “research” purposes. I noted that the word “research” appears nowhere in CASA’s functions in the Civil Aviation Act. (CASA does have the function of, for example, cooperating with the Australian Transport Safety Bureau in relation to investigations under the TSI Act that relate to aircraft, and the ATSB can compel CASA to provide medical information about us in the course an investigation. There’s no deidentification required in that case, for obvious reasons.) CASA doesn’t have the corporate competence to do the jobs that are actually stated in the Civil Aviation Act – among the elephants in that room is “developing … concise aviation safety standards” – so better to focus on those than chasing medical research butterflies.
In essence, the CASA person’s response is that CASA has the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not.
I have raised this issue, among related issues, with the Office of the Australian Information Commissioner (OAIC).
Assuming CASA does have the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not, it raises the question as to effectiveness of the procedures used in fact by CASA to achieve deidentification. (The OAIC has much to say on deidentification.) Given my first-hand experience in AAT matters against CASA and the content of CASA documents, disclosed under FOI, about how Avmed conducts itself, I have little faith in the effectiveness of whatever little governance arrangements are placed around Avmed’s activities.
I have submitted FOI requests to CASA in the following terms on Friday (18 Aug 2023):
I will keep everyone informed of the OAIC’s response and the outcomes of my FOI requests.
Because of my concern for aviation safety in the real world, where Avmed’s increasingly overreaching behaviour is resulting in pilots being increasingly unwilling to disclose information to Avmed and – worse still – to seek medical advice on potential issues for fear that it will get back to Avmed – an outcome inimical to aviation safety - I entered into some correspondence with CASA’s privacy folk recently. My correspondence was precipitated by my recollection that, years ago, there was a ‘tick box’, on the medical certificate application form, which you could tick to consent to the information in the form being used in medical studies. That tick box has gone. These days we’re apparently simply “acknowledging” that our information – “deidentified” – can be used in “research” (and “internal audit”).
(This is one of the many reasons for my description of us medical certificate applicants as “guinea pigs”. Each time we’re sent off to some expensive and sometimes risky tests which qualified specialists say are not justified, it appears we’re providing more data to Avmed for “research”. My educated guess is that the results of the “research” are used to justify Avmed’s own existence and the ‘need’ to intrude into the ‘management’ of the ever-increasing number of ‘aero-medically relevant’ conditions they keep discovering. I anticipate the results are also the subject of Avmed conference echo chambers.)
For my part, I disclose my information for the purpose of, and only for the purpose of, being assessed against the statutory criteria for the issue of a medical certificate. I either meet those criteria or I don’t, and whether my information – deidentified or otherwise – is used in research is irrelevant to that question.
In essence, I asked how CASA got the job of using or disclosing our deidentified sensitive medical information for “research” purposes. I noted that the word “research” appears nowhere in CASA’s functions in the Civil Aviation Act. (CASA does have the function of, for example, cooperating with the Australian Transport Safety Bureau in relation to investigations under the TSI Act that relate to aircraft, and the ATSB can compel CASA to provide medical information about us in the course an investigation. There’s no deidentification required in that case, for obvious reasons.) CASA doesn’t have the corporate competence to do the jobs that are actually stated in the Civil Aviation Act – among the elephants in that room is “developing … concise aviation safety standards” – so better to focus on those than chasing medical research butterflies.
In essence, the CASA person’s response is that CASA has the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not.
I have raised this issue, among related issues, with the Office of the Australian Information Commissioner (OAIC).
Assuming CASA does have the function of using and disclosing our deidentified sensitive medical information for research purposes, and CASA can do that whether we consent to it or not, it raises the question as to effectiveness of the procedures used in fact by CASA to achieve deidentification. (The OAIC has much to say on deidentification.) Given my first-hand experience in AAT matters against CASA and the content of CASA documents, disclosed under FOI, about how Avmed conducts itself, I have little faith in the effectiveness of whatever little governance arrangements are placed around Avmed’s activities.
I have submitted FOI requests to CASA in the following terms on Friday (18 Aug 2023):
I will keep everyone informed of the OAIC’s response and the outcomes of my FOI requests.
Imagine how incorrect the data would be. As simple as the alcohol questions or mental health. They would be using it to make future decisions based that dataset.
It's about time we didn't have to fear for our jobs by them telling the truth. It's a joke of a system.
It's about time we didn't have to fear for our jobs by them telling the truth. It's a joke of a system.
The following users liked this post:
A joke of a system
Imagine the $millions wasted, and time wasted, with optometrist reports and various medical specialists.
Not to mention the great danger to the public by having all these health questionable pilots out there on our crowded roads to and fro numbers of medical examination appointments. Must be risky because CASA would have an evidential risk assessment of incapacitation events. I must look that up in CASA’s website.
The following users liked this post:
Thread Starter
An expensive joke that’s not funny. Ladloy highlights the facade. Avmed doesn’t have a “complete history” of many pilots, septugenarian, because many pilots withhold information, or don’t seek medical advice when in doubt, for (legitimate and reasonable) fear of Avmed’s damaging overreactions. And they’re using the data gathered for research.
Setting aside trivial issues like the lawfulness and ethics of what Avmed’s doing, it’s having perverse consequences.
Setting aside trivial issues like the lawfulness and ethics of what Avmed’s doing, it’s having perverse consequences.
AVMED research?
Whatever research AVMED may be carrying out it cannot be anything relevant to the safety of flight. The low weight RAAus and Gliding Federation successful self declared system across 40 and some 70 years respectively are testament to AVMED’s complete lack of reality.
For meaningful statistics we now have some from the USA.
For meaningful statistics we now have some from the USA.
The following users liked this post:
Every pilot I know has their normal doc and their DAME and they don’t know about the other.
dunno what sort of dataset that will give you. But any research paper should acknowledge that limitation
Perversely, a “Class 1 pilots are really healthy compared to the general population “ conclusion (as so much is hidden from AVMED) might be self validating AVMED’s approach.
dunno what sort of dataset that will give you. But any research paper should acknowledge that limitation
Perversely, a “Class 1 pilots are really healthy compared to the general population “ conclusion (as so much is hidden from AVMED) might be self validating AVMED’s approach.
Last edited by compressor stall; 30th Sep 2023 at 04:20.
The following users liked this post:
Thread Starter
It might be, but only if one subscribes to causation for Martians.
The following users liked this post: