


Empire Strikes Back! on Colour Defective Pilots... Again.

Thread Starter
Empire Strikes Back! on Colour Defective Pilots... Again.
It's been discussed in some other threads recently that CASA have changed the way they deal with CVD pilots. Given the importance of this issue to so many current and aspiring pilots, I have started this new thread to highlight the topic and offer perspective on behalf of the Colour Vision Defective Pilots Association (CVDPA).
10 years on from the Empire Strikes Back! on Colour Defective Pilots saga and the dark days of the AvMed Navathe era, it disappoints me to see that we're back here again. At the time, that PPRuNe thread ran for 36 pages and was highly successful in raising awareness of the plight of CVD pilots and our unjust treatment by AvMed zealots at the time.
After my own AAT win in 2014 (and two previous AAT wins in the late 1980s) it seemed like we were finally making progress, albeit slowly. New Zealand led the way with the introduction of the Operational Colour Vision Assessment (OCVA) and there was a brief period of enlightenment in Australia during 2020-2021 when former CASA CEO Shane Carmody and former PMO Dr Simon May followed NZ's lead and implemented the OCVA here too. Myself and many others were finally able to progress our careers to the fullest extent possible and get on with our lives again.
When CVDPA learnt in early 2022 that CASA had suspended the OCVA due to apparent concerns around lack of standardisation, we contacted the new PMO Dr Kate Manderson. She responded via email on 18/01/22 and advised:
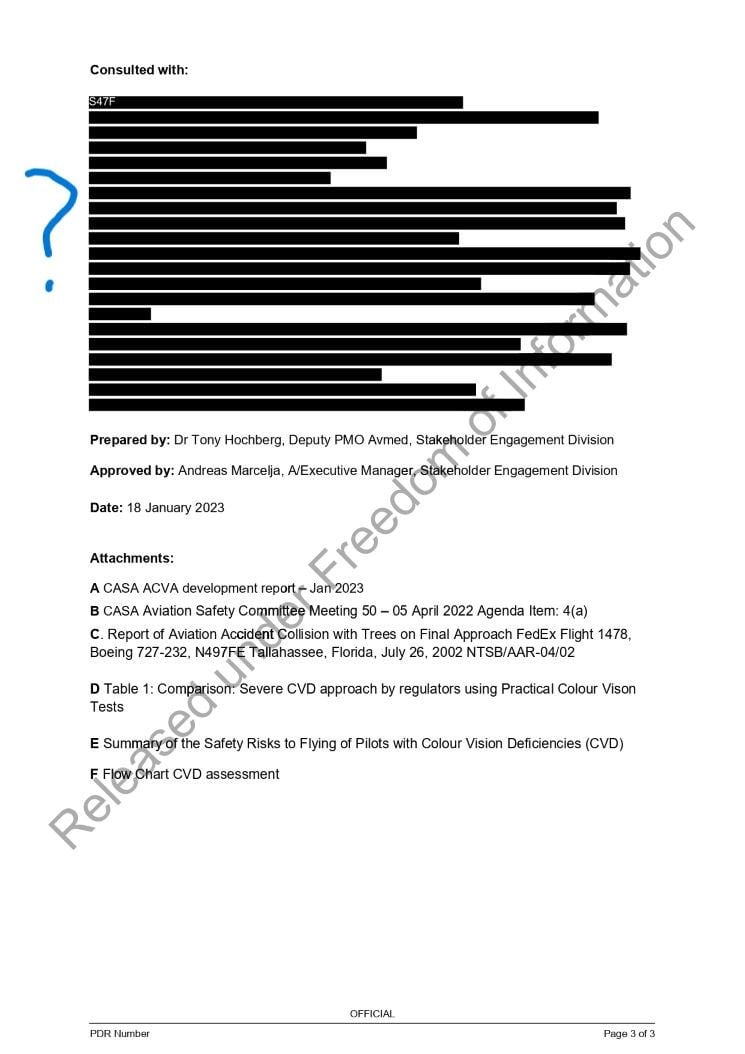
This all sounded quite positive and despite early indications from the PMO that she wanted CVDPA to be involved in the working group tasked with reviewing the OCVA, we were quickly excluded from the process when the Deputy PMO Dr Tony Hochberg took over as the project manager and filled it with medical 'experts'. As of today, we still have no knowledge of the persons comprised in this panel (this information was redacted in recent documents obtained under FOI). However, I'd be willing to bet that at least some involved stand to make money out of the continued administration of clinical CVD tests, including the CAD.
Despite this, we continued to work proactively with CASA in an attempt to achieve a timely and satisfactory resolution. However, almost 2 years after the OCVA was suspended, it has become increasingly clear in recent months that AvMed wish to return us to the dark ages again and have proposed including restrictions on pilots' medicals, even if they pass the new test - to be renamed the ACVA. They're also refusing to recognise the pass results of some candidates who passed the original OCVA in the months leading up to it's suspension.
During the recent Senate Estimates hearing, CASA provided advice to Senator David Fawcett that this was incorrect:
The responses provided during Estimates are contrary to the advice that CVDPA has been given by CASA in their communications with us and also contradict information contained in documents recently obtained under FOI, which make it abundantly clear that the AvMed seek to continue to impose restrictions on CVD pilots. CVDPA have raised our concerns directly with CEO Pip Spence and yet 7 weeks on, our emails have gone unanswered.
We can only hope that she is using this time to get the zealots back in check. Stay tuned for more!
John O'Brien
CVDPA
10 years on from the Empire Strikes Back! on Colour Defective Pilots saga and the dark days of the AvMed Navathe era, it disappoints me to see that we're back here again. At the time, that PPRuNe thread ran for 36 pages and was highly successful in raising awareness of the plight of CVD pilots and our unjust treatment by AvMed zealots at the time.
After my own AAT win in 2014 (and two previous AAT wins in the late 1980s) it seemed like we were finally making progress, albeit slowly. New Zealand led the way with the introduction of the Operational Colour Vision Assessment (OCVA) and there was a brief period of enlightenment in Australia during 2020-2021 when former CASA CEO Shane Carmody and former PMO Dr Simon May followed NZ's lead and implemented the OCVA here too. Myself and many others were finally able to progress our careers to the fullest extent possible and get on with our lives again.
When CVDPA learnt in early 2022 that CASA had suspended the OCVA due to apparent concerns around lack of standardisation, we contacted the new PMO Dr Kate Manderson. She responded via email on 18/01/22 and advised:
This is something that came up in December last year, and we are still working through what the issues are and how they impact on people who have submitted their assessments recently, and what we need to do to be able to make sure the OCVA is acceptable and its results can’t be questioned in the future. Please be assured, there is no change to CASA policy, the OCVA is here to stay. These issues are, I hope, going to push us along so that the OCVA is as strong as it can possibly be for the longer term, and perhaps even for other jurisdictions.
This all sounded quite positive and despite early indications from the PMO that she wanted CVDPA to be involved in the working group tasked with reviewing the OCVA, we were quickly excluded from the process when the Deputy PMO Dr Tony Hochberg took over as the project manager and filled it with medical 'experts'. As of today, we still have no knowledge of the persons comprised in this panel (this information was redacted in recent documents obtained under FOI). However, I'd be willing to bet that at least some involved stand to make money out of the continued administration of clinical CVD tests, including the CAD.
Despite this, we continued to work proactively with CASA in an attempt to achieve a timely and satisfactory resolution. However, almost 2 years after the OCVA was suspended, it has become increasingly clear in recent months that AvMed wish to return us to the dark ages again and have proposed including restrictions on pilots' medicals, even if they pass the new test - to be renamed the ACVA. They're also refusing to recognise the pass results of some candidates who passed the original OCVA in the months leading up to it's suspension.
During the recent Senate Estimates hearing, CASA provided advice to Senator David Fawcett that this was incorrect:
Ms Spence : I think what we're saying is that we think our website's wrong. We will go back to review it, because that doesn't sound like our policy. As Dr Manderson said, we're working—and we're working internationally—looking at how we manage this issue. But the whole point, in the simplest terms, was that if you pass the test then you've got a permission to fly. Those sorts of conditions you've just described should not be applying. If you can bear with us, we'll review the website, because what you've read out just doesn't sound right.
The responses provided during Estimates are contrary to the advice that CVDPA has been given by CASA in their communications with us and also contradict information contained in documents recently obtained under FOI, which make it abundantly clear that the AvMed seek to continue to impose restrictions on CVD pilots. CVDPA have raised our concerns directly with CEO Pip Spence and yet 7 weeks on, our emails have gone unanswered.
We can only hope that she is using this time to get the zealots back in check. Stay tuned for more!
John O'Brien
CVDPA
Last edited by johnobr; 6th Nov 2023 at 10:13.

The following 6 users liked this post by johnobr:
Thread Starter
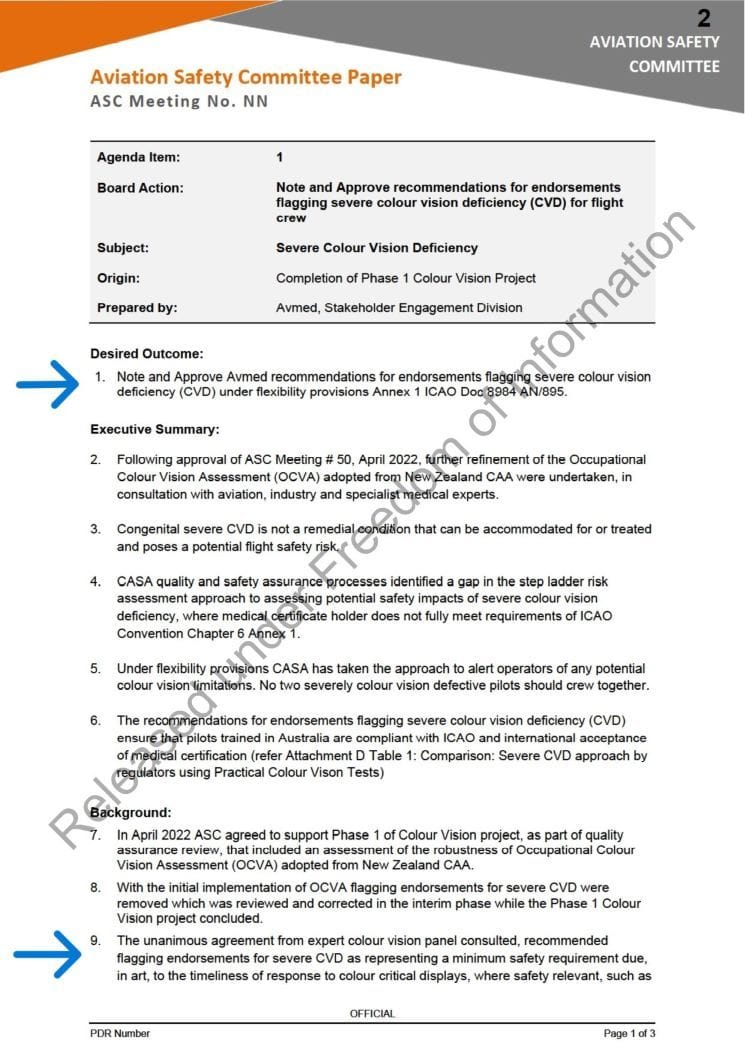
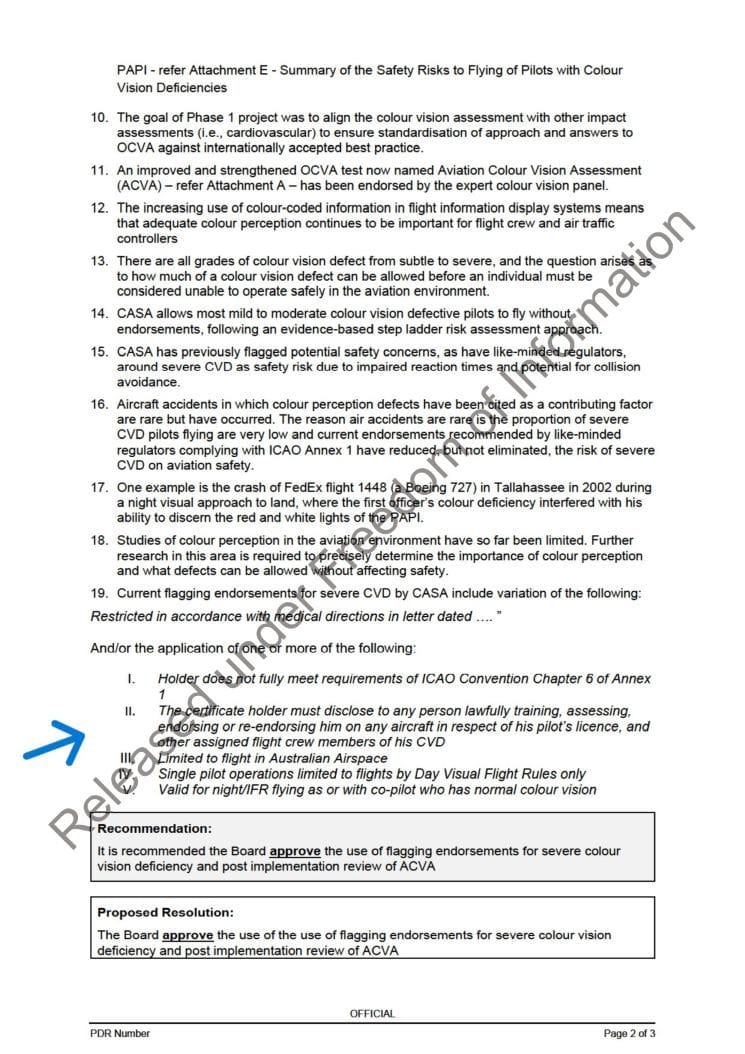
In case anyone's in any doubt about CASA's true intentions to wind back the clock again, the below Aviation Safety Committee Paper from 18/01/23 obtained under FOI is revealing.
During Estimates questioning, the Exec Manager Stakeholder Engagement advised:
Interestingly, the CASA website was updated after Estimates to remove mention of the proposed restrictions, but perhaps Mr Marcelja forgot that he approved this paper (prepared by Dr Hochberg)?
During Estimates questioning, the Exec Manager Stakeholder Engagement advised:
Mr Marcelja: Could I jump in? The website and some of that information sits in my area. I think what you're describing, if that is correct, is not our policy. Our policy is that there are various conditions that we can put on medical certificates, depending on how you go in the test, but if you pass the test and can demonstrate that you're operationally safe there is no condition of a copilot. What Dr Manderson is saying, though, is that, because you have not met a medical standard that's internationally accepted but have proven you are safe, we will grant you a medical certificate. We can't say that you've met a standard but we can say you're safe to fly, and those conditions will be applied depending on the way you've gone. If that's on our website, I'll take that up, because that's not the policy.
The following 4 users liked this post by johnobr:
How frustrating listening to these people!
The Senator: "Where is the evidence?"
CASA..."erm, that doesn't sound right"
A quick look at Google Scholar shows plenty of literature on the subject but have CASA ever given any references to scientific evidence?
What is attachment E? Doesn't look like a reference to me.
The Senator: "Where is the evidence?"
CASA..."erm, that doesn't sound right"
A quick look at Google Scholar shows plenty of literature on the subject but have CASA ever given any references to scientific evidence?
What is attachment E? Doesn't look like a reference to me.
The following is my prediction of what’s going on with the Australian Colour Vision Assessment (ACVA) and why.
What CASR says
It is first necessary to understand what the CASRs say about the way in which a candidate must demonstrate compliance with the colour perception criterion in the class 1 and class 2 medical standards. I’ll quote the provisions relevant to the class 1 standard, but the provisions are effectively identical for the class 2 standard.
The criteria for the class 1 medical standard are in table 67.150. Item 1.39 of that table is the ‘colour perception’ criterion. That item says:
Note: For how to demonstrate this, see subregulation 67.150(6).
This is what CASR 67.150(6) says:
(a) in daylight, or artificial light of similar luminosity, readily identifying a series pseudo‑isochromatic plates of the Ishihara 24‑plate type, making no more than 2 errors; or
(b) for somebody who makes more than 2 errors in a test mentioned in paragraph (a), readily identifying aviation coloured lights displayed by means of a Farnsworth colour‑perception lantern, making:
(i) no errors on 1 run of 9 pairs of lights; or
(ii) no more than 2 errors on a sequence of 2 runs of 9 pairs of lights; or
(c) for somebody who does not satisfy paragraph (a) or (b), correctly identifying all relevant coloured lights in a test, determined by CASA, that simulates an operational situation.
The plain words of CASR 67.150(6) are quite simple.
If a candidate gets a tick in the (a) box – the ‘first tier’ test – the candidate has demonstrated compliance with the colour perception criterion in the standard.
If a candidate gets a cross in the (a) box but a tick in (b) box – the ‘second tier’ test – the candidate has still demonstrated compliance with the colour perception criterion in the standard.
If a candidate gets a cross in the (a) box and a cross in the (b) box but a tick in the (c) box – the ‘third tier’ text – the candidate has still demonstrated compliance with the colour perception criterion in the standard.
As we’ll see, that plain meaning of those words is inconvenient to the CVD zealots and, therefore, the CVD zealots have been busily trying to create a structure to subvert and avoid that plain meaning. But first we need to understand what happened during the brief period of enlightenment after the Operational Colour Vision Assessment (OCVA) – championed by the NZ CAA in the face the CVD zealots – was implemented in Australia.
The brief period of enlightenment in Australia – the OCVA
The implementation of the OCVA in Australia brought an end to the crusade led by CVD zealot Navathe. He spearheaded the crusade which included letters sent to air operators about the presence of the unclean, dangerous CVD crew in their workforce. He also introduced the ‘CAD test’ as a purported test simulating an operational situation.
(I say ‘purported’ because – despite the sophistry I’ve read in various items of CASA correspondence – no court has ever found the CAD to be a validly determined ‘third tier’ test. Only zealots blinded by their noble cause could characterise the CAD as a test simulating an operational situation. For those not blinded by prejudice, the CAD test merely confirms what is already known about the candidate and simulates no operational situation known to pilots. And – hardly surprisingly, given the lack of corporate governance in CASA – my recent FOI request for access to the current document of determination of the CAD as a ‘third tier’ test by a delegate of the power to do that produced no document of determination by a delegate of the CAD as a ‘third tier’ test. The zealots are above all that pesky accountability stuff.)
Then the OCVA was implemented as a ‘third tier’ test. Enlightenment! (In fact, it was just a shift to compliance with the existing law, in the face of the wailing and gnashing of CVD zealot teeth.)
During the period of enlightenment:
- Candidates could choose to undergo the OCVA instead of the CAD. They of course usually chose the OCVA because it’s productive flying rather than an expensive test that reveals something the candidate already knows.
- Candidates who passed the OCVA were issued ‘clean’ medical certificates so far as colour vision was concerned. That is, after all, the consequence of having demonstrated compliance with the colour perception criterion in accordance with the law.
A return to the dark ages, again
Sadly, a change of personnel in CASA led to an opportunity for the CVD zealots to regroup and recommence their crusade. The recommencement was justified on the pretext of some concocted ‘new’ evidence of the dire consequences of CVD and the inadequacy of the OCVA.
Dr Manderson and Dr Hochberg said around 18 months ago that “it is determined that additional investment and leadership is now required to refine this assessment tool [the OCVA], and strengthen the OCVA as a reliable, defensible, and effective colour vision assessment for aviation, including in international jurisdictions”. Makes you feel safer already, doesn’t it, knowing these self-appointed leaders are going to refine and strengthen the OCVA?
Everyone was under the impression that the ‘refined and strengthened OCVA’ would supersede the original OCVA as a ‘third tier’ test. That’s exactly what people were told by CASA, after all. And it’s actually the only option accommodated by a thing called ‘the law’.
The zealots then set up a little echo chamber of people - whose identities and business interests have not been disclosed under FOI – to ‘refine and strengthen’ the OCVA. At some point along the way the name changed to the Australian Colour Vision Assessment (ACVA) presumably to recognise the selfless leadership of the CASA zealots and the invitees to its echo chamber.
But then the zealots had a Hotel Sierra Mike. They realised that if the ACVA were a ‘third tier’ test, there would be unacceptable outcomes for the zealots:
- Candidates could choose to do the ACVA instead of the CAD. That would deprive the zealots of CAD data to analysis and discuss in their echo chamber, and the administrators of the CAD would be deprived of income.
- Candidates who pass the ACVA would have demonstrated compliance with the colour perception criterion and therefore be entitled to a ‘clean’ medical certificate so far as colour perception goes.
That is anathema to the zealots! In their world, candidates with CVD must be outed, labelled and restricted. There are no other alternatives in their religion.
So what are the zealots trying to do, and have been discovered doing, so as to subvert and avoid the plain words of CASR? They’ve decided that they will try to ‘policy’ their way around the law.
I’ve seen it in black and white in recent CASA correspondence: “It is … Avmed policy that before consideration can be given to accepting an OCVA style test conducted in an aircraft, a recognised third level test – such as the CAD test – must have been undertaken and the results provided to Avmed.”
Brilliant! They’ve conjured up a non-existent ‘fourth tier’ for the ACVA. That way:
- The candidates have failed to demonstrate compliance with the colour vision criterion because they’ve failed the CAD (and the first and second tier tests).
- The providers of the CAD test continue to get income from administering it.
- The zealots continue to get data from the CAD test to feed their echo chamber.
- The candidates then become the plaything of AvMed’s “endorsements” (restrictions) and the ACVA becomes another data-gathering exercise and a means by which AvMed will decide how much the victims will be restricted.
(By they way: They also conjured up a ‘second tier’ test that isn’t actually in the regulations: The ‘Optec 900’. It will be interesting to find out who makes money out of administering that test and whether they were invited to participate in the echo chamber.)
This all fits within my definition of corruption. Public officials going out of their way to subvert and avoid the law, in pursuit of their noble cause. Opaque processes, undisclosed participants and misleading information propagated along the way. And the interests of pilots and aspiring pilots – and the hundreds of thousands of people with CVD in Australia - be damned.
I expect the zealots will now blame the likes of Senator Fawcett and the CVDPA for further delays in the unveiling of the ‘refined and strengthened’ masterpiece the ACVA, for having had the temerity – the utter gall – to expect public officials to be transparent in and accountable for their activities.
It’s now a test of Ms Spence and the CASA Board. Will they rally around and support the zealots? Or will they require the law to be administered in accordance with its plain terms?
By the way: I do not have CVD.
What CASR says
It is first necessary to understand what the CASRs say about the way in which a candidate must demonstrate compliance with the colour perception criterion in the class 1 and class 2 medical standards. I’ll quote the provisions relevant to the class 1 standard, but the provisions are effectively identical for the class 2 standard.
The criteria for the class 1 medical standard are in table 67.150. Item 1.39 of that table is the ‘colour perception’ criterion. That item says:
Can readily distinguish the colours that need to be distinguished for the safe exercise of privileges, or performance of duties, under the relevant licence.
Note: For how to demonstrate this, see subregulation 67.150(6).
(6) A person must demonstrate that he or she meets the criterion in item 1.39 of table 67.150 by:
(a) in daylight, or artificial light of similar luminosity, readily identifying a series pseudo‑isochromatic plates of the Ishihara 24‑plate type, making no more than 2 errors; or
(b) for somebody who makes more than 2 errors in a test mentioned in paragraph (a), readily identifying aviation coloured lights displayed by means of a Farnsworth colour‑perception lantern, making:
(i) no errors on 1 run of 9 pairs of lights; or
(ii) no more than 2 errors on a sequence of 2 runs of 9 pairs of lights; or
(c) for somebody who does not satisfy paragraph (a) or (b), correctly identifying all relevant coloured lights in a test, determined by CASA, that simulates an operational situation.
If a candidate gets a tick in the (a) box – the ‘first tier’ test – the candidate has demonstrated compliance with the colour perception criterion in the standard.
If a candidate gets a cross in the (a) box but a tick in (b) box – the ‘second tier’ test – the candidate has still demonstrated compliance with the colour perception criterion in the standard.
If a candidate gets a cross in the (a) box and a cross in the (b) box but a tick in the (c) box – the ‘third tier’ text – the candidate has still demonstrated compliance with the colour perception criterion in the standard.
As we’ll see, that plain meaning of those words is inconvenient to the CVD zealots and, therefore, the CVD zealots have been busily trying to create a structure to subvert and avoid that plain meaning. But first we need to understand what happened during the brief period of enlightenment after the Operational Colour Vision Assessment (OCVA) – championed by the NZ CAA in the face the CVD zealots – was implemented in Australia.
The brief period of enlightenment in Australia – the OCVA
The implementation of the OCVA in Australia brought an end to the crusade led by CVD zealot Navathe. He spearheaded the crusade which included letters sent to air operators about the presence of the unclean, dangerous CVD crew in their workforce. He also introduced the ‘CAD test’ as a purported test simulating an operational situation.
(I say ‘purported’ because – despite the sophistry I’ve read in various items of CASA correspondence – no court has ever found the CAD to be a validly determined ‘third tier’ test. Only zealots blinded by their noble cause could characterise the CAD as a test simulating an operational situation. For those not blinded by prejudice, the CAD test merely confirms what is already known about the candidate and simulates no operational situation known to pilots. And – hardly surprisingly, given the lack of corporate governance in CASA – my recent FOI request for access to the current document of determination of the CAD as a ‘third tier’ test by a delegate of the power to do that produced no document of determination by a delegate of the CAD as a ‘third tier’ test. The zealots are above all that pesky accountability stuff.)
Then the OCVA was implemented as a ‘third tier’ test. Enlightenment! (In fact, it was just a shift to compliance with the existing law, in the face of the wailing and gnashing of CVD zealot teeth.)
During the period of enlightenment:
- Candidates could choose to undergo the OCVA instead of the CAD. They of course usually chose the OCVA because it’s productive flying rather than an expensive test that reveals something the candidate already knows.
- Candidates who passed the OCVA were issued ‘clean’ medical certificates so far as colour vision was concerned. That is, after all, the consequence of having demonstrated compliance with the colour perception criterion in accordance with the law.
A return to the dark ages, again
Sadly, a change of personnel in CASA led to an opportunity for the CVD zealots to regroup and recommence their crusade. The recommencement was justified on the pretext of some concocted ‘new’ evidence of the dire consequences of CVD and the inadequacy of the OCVA.
Dr Manderson and Dr Hochberg said around 18 months ago that “it is determined that additional investment and leadership is now required to refine this assessment tool [the OCVA], and strengthen the OCVA as a reliable, defensible, and effective colour vision assessment for aviation, including in international jurisdictions”. Makes you feel safer already, doesn’t it, knowing these self-appointed leaders are going to refine and strengthen the OCVA?
Everyone was under the impression that the ‘refined and strengthened OCVA’ would supersede the original OCVA as a ‘third tier’ test. That’s exactly what people were told by CASA, after all. And it’s actually the only option accommodated by a thing called ‘the law’.
The zealots then set up a little echo chamber of people - whose identities and business interests have not been disclosed under FOI – to ‘refine and strengthen’ the OCVA. At some point along the way the name changed to the Australian Colour Vision Assessment (ACVA) presumably to recognise the selfless leadership of the CASA zealots and the invitees to its echo chamber.
But then the zealots had a Hotel Sierra Mike. They realised that if the ACVA were a ‘third tier’ test, there would be unacceptable outcomes for the zealots:
- Candidates could choose to do the ACVA instead of the CAD. That would deprive the zealots of CAD data to analysis and discuss in their echo chamber, and the administrators of the CAD would be deprived of income.
- Candidates who pass the ACVA would have demonstrated compliance with the colour perception criterion and therefore be entitled to a ‘clean’ medical certificate so far as colour perception goes.
That is anathema to the zealots! In their world, candidates with CVD must be outed, labelled and restricted. There are no other alternatives in their religion.
So what are the zealots trying to do, and have been discovered doing, so as to subvert and avoid the plain words of CASR? They’ve decided that they will try to ‘policy’ their way around the law.
I’ve seen it in black and white in recent CASA correspondence: “It is … Avmed policy that before consideration can be given to accepting an OCVA style test conducted in an aircraft, a recognised third level test – such as the CAD test – must have been undertaken and the results provided to Avmed.”
Brilliant! They’ve conjured up a non-existent ‘fourth tier’ for the ACVA. That way:
- The candidates have failed to demonstrate compliance with the colour vision criterion because they’ve failed the CAD (and the first and second tier tests).
- The providers of the CAD test continue to get income from administering it.
- The zealots continue to get data from the CAD test to feed their echo chamber.
- The candidates then become the plaything of AvMed’s “endorsements” (restrictions) and the ACVA becomes another data-gathering exercise and a means by which AvMed will decide how much the victims will be restricted.
(By they way: They also conjured up a ‘second tier’ test that isn’t actually in the regulations: The ‘Optec 900’. It will be interesting to find out who makes money out of administering that test and whether they were invited to participate in the echo chamber.)
This all fits within my definition of corruption. Public officials going out of their way to subvert and avoid the law, in pursuit of their noble cause. Opaque processes, undisclosed participants and misleading information propagated along the way. And the interests of pilots and aspiring pilots – and the hundreds of thousands of people with CVD in Australia - be damned.
I expect the zealots will now blame the likes of Senator Fawcett and the CVDPA for further delays in the unveiling of the ‘refined and strengthened’ masterpiece the ACVA, for having had the temerity – the utter gall – to expect public officials to be transparent in and accountable for their activities.
It’s now a test of Ms Spence and the CASA Board. Will they rally around and support the zealots? Or will they require the law to be administered in accordance with its plain terms?
By the way: I do not have CVD.
The following 6 users liked this post by Clinton McKenzie:
Thread Starter
CAD test... simulating an operational situation?
And just in case anyone needs reminding of what the CAD (Colour Assessment & Diagnosis) test looks like, here it is:
Yep - this is what the AvMed zealots are currently using to satisfy CASR 67.150 (6)(c) - a test which is required under the law to simulate an operational situation.
Even the inventor of the test, Professor John Barbur, who gave evidence during my AAT appeal refuted this proposition:

Yep - this is what the AvMed zealots are currently using to satisfy CASR 67.150 (6)(c) - a test which is required under the law to simulate an operational situation.
Even the inventor of the test, Professor John Barbur, who gave evidence during my AAT appeal refuted this proposition:
“…Like in every study there are sort of strengths and weaknesses. The CAD system is mainly wasn’t designed specifically for aviation. It was designed for assessing colour vision, for detecting deficiency, both congenital as well as acquired, for quantifying the severity of colour vision loss, and for classifying accurately the class of colour deficiency involved. So from that point of view the CAD test, which is based on findings from camouflage studies some 25 years ago is an extremely good colour vision test and that’s as far as we go.”
“Yes, I mean the CAD test was not intended in any way to use direct information on operational tasks. What the CAD test does is to measure the colour signal strength. One needs to see red/green and yellow/blue colours and it does so very efficiently. If one doesn’t have colour vision one simply cannot carry out a test…”
“So that’s what the CAD test is. Just because it happens to predict a level of severity beyond which one cannot be considered safe within a particular environment. That does not make the CAD an operational test.”
The following 3 users liked this post by johnobr:
The following 3 users liked this post by Bill Smith:

For me this is a case of �long time listener, first time caller� and my first post on PPruNe after many years lurking in the shadows, I am now driven to action having watched CASA�s performance (and that�s exactly what it was�a performance) at Senate Estimates.
I felt it time for me to offer a critical review, so if you will indulge me for just a moment, my movie review would go something along the lines of:
�A masterclass in manipulation. Whilst appearing to make logical arguments, the chief protagonists expertly distort reality, creating a false narrative that is so believable, that even critical minds would be forgiven for believing elements of fiction. The viewer is at times unsure whether to laugh or cry. Sophistry in its purest form. 4 stars�
So amateur movie review out of the way�let�s dive deeper.
Sophistry - what even is that?
Other than a word I�ve found myself with increasing frequency this year, sophistry is defined as:
�the clever use of arguments that seem true but are really false, in order to deceive people�
In this instance, deceive people that:
The Legislative Contest � Air Law 101
I�m not a lawyer, and short of a few subjects at university many years ago have no legal training, however this should really be a refresher for anyone who has done CPL Air Law.
In Australia, our standards (Medical, Flight Crew Licencing, Maintenance, General Operating & Flight Rules) are defined in the Civil Aviation Safety Regulations (CASR). This legislation is what the regulator (CASA) enforces.
For the purposes of this discussion � Part 67 (Medical Standards) is the most relevant. It is the Standard to which all Australian medicals are issued.
Ok, fine I hear you say�what�s the big deal about all of that? Well it�s important background to the first fallacy masquerading as truth, and that is�..
The myth of the �International Medical Standard�
ICAO as an international organisation, sets out the high-level standards for member states to review, refine and implement in their own jurisdictions. As a sovereign nation � Australia has adopted and codified the ICAO standards, as they apply to aviation in this country, and it is this which has found its way into the CASRs.
Whatever ICAO may include and amend from time to time in their standard � is not legally binding or enforceable in its own right, or relevant when it comes to making decisions in the Australian context. The only thing that is relevant is the content of the CASR�s that are enshrined in Australian law.
Which means�wait for it� every ICAO member state has implemented these standards and recommended practices differently. In fact, this is normal. Each member state is required to publish a document stating where and how they differ from the ICAO standard ore recommended practice. It�s so normal that there is an established process for it!
In fact, there are 19 different annexes which cover 209 pages of differences to the ICAO standards and what is implemented in Australia that are published and buried in the AIP.
Annex 1 is the relevant one here � as covers personnel licensing (including medical standards). As of the time of this post there are 26 pages of differences in that Annex alone, with 86 individual references to differences in the medical standards.
So�with almost half a reem of paper worth of differences to the ICAO standard�.how�s that inviolable �international standard� holding up? It's OK... We're not done talking about 'standards' just yet!
The false narrative that there is a �Medical Standard� and a �Practical Standard�.
I really like this one, if you can�t beat them�create a new club of your own. In this case, create a narrative that there are two different types of standard by defining a new type of standard, that way you can decide how it gets treated�despite what the CASR says!
Let�s look at how AVMED are positioning this. A blanket assertion that pilots with CVD do not meet the standard despite there being 3 tiers of testing defined with a pass of any of these tiers meeting the standard for a �clean� medical issue, and trying to limit �Medical� to clinical testing only:
This is a clear attempt to create a concept of two �standards�, so that additional restrictions can be placed on pilots with CVD, who would otherwise pass a practical, flight-based assessment of their colour vision.
Fact Check: There is only ONE medical standard, and that is the one defined in Part 67 of the CASR.
OCVA flight test consistency � a Trojan Horse of a problem
Let�s firstly look at the problems with the OCVA test as described by AVMED:
Ok, that�s the problem statement. So let�s look at how this has been addressed in an appropriate and proportionate manner:
This isn�t a big task, especially when you take into consideration that that there were only ever 28 examiners trained and accredited by AVMED to complete OCVA testing. It becomes an even easier task when you take into account that only 8 examiners have ever conducted these flight tests. I�ve managed bigger WhatsApp groups than that!
From the outside looking in, this really looks like the hijacking of a convenient issue, to drive another agenda that was the complete redesign of the operational flight test. In no other cases would consistency issue with a flight test be handled in such a way.
Bending of the truth � understating the real impact on people�s lives
The final, and perhaps most insidious bending of the truth has to be one of the final statements made by AVMED:
I�m sure this statement is 100% factually correct. However we must look carefully at the wording here, as there are many things CASA can do to destroy a career or livelihood, or even dreams of aspiring pilots without cancelling or refusing to issue a medical. And the obvious one is conditions.
CASA could technically issue a medical subject to the condition that the pilot could only ever operate on the 31st day of every month, where that day fell on a Tuesday, and only whilst wearing pink polka dot Oodie. Now fashion crimes aside, that would limit you to flying 2 days this year - but would not be considered a cancellation or refusal.
Issuing a medical with restrictions such as �DAY VFR ONLY�, �ONLY VALID AS OR WITH A COPILOT WHO HAS NO CVD� or �NO PASSENGERS AT NIGHT� severely limits and restricts pilots with, and AVMED have been quietly busying themselves with adding these restrictions to pilots with CVD and existing medicals as and when they can. I personally know at least one in this circumstance right now.
Final thoughts and disclosures
It appears clear that CASA are ramping up the fight (again) on pilots with CVD, and doing so in a way which is not just intellectually, but also morally dishonest.
From the construction of arguments trying to divorce what the actual medical standards are and what officials in CASA would rather they be, to using �consistency issues� in a test administration by a group of 8 examiners as rationale to completely redesign it from the ground up, It is becomingly clear that personally desired outcomes are being put ahead of due process, and transparency.
Disclosure: I am a pilot with CVD.
I felt it time for me to offer a critical review, so if you will indulge me for just a moment, my movie review would go something along the lines of:
�A masterclass in manipulation. Whilst appearing to make logical arguments, the chief protagonists expertly distort reality, creating a false narrative that is so believable, that even critical minds would be forgiven for believing elements of fiction. The viewer is at times unsure whether to laugh or cry. Sophistry in its purest form. 4 stars�
So amateur movie review out of the way�let�s dive deeper.
Sophistry - what even is that?
Other than a word I�ve found myself with increasing frequency this year, sophistry is defined as:
�the clever use of arguments that seem true but are really false, in order to deceive people�
In this instance, deceive people that:
- There is a single, golden international medical standard to which we are inextricably bound
- CVD pilots do not and cannot meet �medical� standards
- The OCVA was so badly broken that it needed to be redone from the ground-up
- Noone has been disadvantaged by the 18month delay (and putative medical certificate restrictions)
The Legislative Contest � Air Law 101
I�m not a lawyer, and short of a few subjects at university many years ago have no legal training, however this should really be a refresher for anyone who has done CPL Air Law.
In Australia, our standards (Medical, Flight Crew Licencing, Maintenance, General Operating & Flight Rules) are defined in the Civil Aviation Safety Regulations (CASR). This legislation is what the regulator (CASA) enforces.
For the purposes of this discussion � Part 67 (Medical Standards) is the most relevant. It is the Standard to which all Australian medicals are issued.
Ok, fine I hear you say�what�s the big deal about all of that? Well it�s important background to the first fallacy masquerading as truth, and that is�..
The myth of the �International Medical Standard�
ICAO as an international organisation, sets out the high-level standards for member states to review, refine and implement in their own jurisdictions. As a sovereign nation � Australia has adopted and codified the ICAO standards, as they apply to aviation in this country, and it is this which has found its way into the CASRs.
Whatever ICAO may include and amend from time to time in their standard � is not legally binding or enforceable in its own right, or relevant when it comes to making decisions in the Australian context. The only thing that is relevant is the content of the CASR�s that are enshrined in Australian law.
Which means�wait for it� every ICAO member state has implemented these standards and recommended practices differently. In fact, this is normal. Each member state is required to publish a document stating where and how they differ from the ICAO standard ore recommended practice. It�s so normal that there is an established process for it!
In fact, there are 19 different annexes which cover 209 pages of differences to the ICAO standards and what is implemented in Australia that are published and buried in the AIP.
Annex 1 is the relevant one here � as covers personnel licensing (including medical standards). As of the time of this post there are 26 pages of differences in that Annex alone, with 86 individual references to differences in the medical standards.
So�with almost half a reem of paper worth of differences to the ICAO standard�.how�s that inviolable �international standard� holding up? It's OK... We're not done talking about 'standards' just yet!
The false narrative that there is a �Medical Standard� and a �Practical Standard�.
I really like this one, if you can�t beat them�create a new club of your own. In this case, create a narrative that there are two different types of standard by defining a new type of standard, that way you can decide how it gets treated�despite what the CASR says!
Andreas Marceljaj: Because you don�t meet the medical standard, a medical standard that is internationally accepted, but you�ve proven that you�re safe � we will grant you a medical certificate. So we can�t say that you�ve met a standard, but we can say that you�re safe to fly, and those conditions will be applied depending on how you�ve gone.
Dr Kate Manderson: They (pilots with CVD) don�t meet the standard, but now we can in very detail and very safely effectively and consistently assess whether or not the way they meet the standard presents a hazard to safe air navigation.
Fact Check: There is only ONE medical standard, and that is the one defined in Part 67 of the CASR.
OCVA flight test consistency � a Trojan Horse of a problem
Let�s firstly look at the problems with the OCVA test as described by AVMED:
Dr Kate Manderson: So we had some difficulties where the forms and the flights were not being conducted consistently, to a consistent standard across the board. Where someone may have one kind of flight or assessment with one assessor and a completely different one with somebody else.
- Immediately stop accepting the OCVA test
- Instruct examiners to longer offer it (long after ceasing to accept it)
- Completely redesign the entire test from the ground up (remove night component, map reading, cockpit instrumentation, terrain identification, powerline and hazard identification) to make it solely about the recognition of PAPI lights by day.
- Spend 18 months trying to find a way to position the test outside the existing legislative structure in the CASRs.
This isn�t a big task, especially when you take into consideration that that there were only ever 28 examiners trained and accredited by AVMED to complete OCVA testing. It becomes an even easier task when you take into account that only 8 examiners have ever conducted these flight tests. I�ve managed bigger WhatsApp groups than that!
From the outside looking in, this really looks like the hijacking of a convenient issue, to drive another agenda that was the complete redesign of the operational flight test. In no other cases would consistency issue with a flight test be handled in such a way.
Bending of the truth � understating the real impact on people�s lives
The final, and perhaps most insidious bending of the truth has to be one of the final statements made by AVMED:
Dr. Kate Manderson: There have been no refusals or cancellations for colour vision deficiency.
CASA could technically issue a medical subject to the condition that the pilot could only ever operate on the 31st day of every month, where that day fell on a Tuesday, and only whilst wearing pink polka dot Oodie. Now fashion crimes aside, that would limit you to flying 2 days this year - but would not be considered a cancellation or refusal.
Issuing a medical with restrictions such as �DAY VFR ONLY�, �ONLY VALID AS OR WITH A COPILOT WHO HAS NO CVD� or �NO PASSENGERS AT NIGHT� severely limits and restricts pilots with, and AVMED have been quietly busying themselves with adding these restrictions to pilots with CVD and existing medicals as and when they can. I personally know at least one in this circumstance right now.
Final thoughts and disclosures
It appears clear that CASA are ramping up the fight (again) on pilots with CVD, and doing so in a way which is not just intellectually, but also morally dishonest.
From the construction of arguments trying to divorce what the actual medical standards are and what officials in CASA would rather they be, to using �consistency issues� in a test administration by a group of 8 examiners as rationale to completely redesign it from the ground up, It is becomingly clear that personally desired outcomes are being put ahead of due process, and transparency.
Disclosure: I am a pilot with CVD.
The following 8 users liked this post by mt747:
My observations:
What we have now is an unholy mess. It takes us back to worse conditions and restrictions than in the 1970's. Dr Manderson and her deputy, Dr Hochberg, are true believers and have learnt nothing from the three AAT outcomes that ultimately led Director Carmody and Dr Simon May to adopt and implement the OCVA.
The purpose of the OCVA test was to satisfy a duly qualified examiner of airmen that a candidate for a medical certificate could identify the information needed to perform a pilot's duties safely. The adoption of the OCVA followed extensive investigation, consultation, and consideration on both sides of the Tasman. Both the CAA NZ and CASA directors had face-to-face meetings with each other and the entire industry. The Aviation Safety Advisory Panel (ASAP) supported implementing the OCVA unanimously.
A pass on the OCVA posed no threat of any description to the safety of air navigation, as it didn't qualify the candidate to perform any task involved in flying an aircraft. It made it possible to study, train and be tested in the same manner as a candidate with normal colour vision. Safe operation performance is a subject that medicos are not qualified to judge. This assessment falls in the domain of professional examiners of airmen.
Finally, I am not against medical standards. The safety implications of heart disease, hypertension, diabetes, and neurological diseases (e.g. epilepsy) are profound. A pilot having a fit, a heart attack, a stroke, or a hypoglycaemic episode is manifestly unlikely to be able to perform their duties as a pilot safely. Defective colour vision has no such dire consequences.
- � "The Empire": a coalition of true believers from various countries that see it as their duty and right to protect and defend the aviation colour perception standard, in the false belief that their actions will enhance the safety of air navigation.
- � Arrogance: an insulting way of thinking or behaving that comes from believing that you are better, smarter, or more important than others. CASA's arrogance on this issue is palpable. They disdain the AAT and the law in general, as well as their immediate predecessors, namely Mr Shane Carmody, Director, Dr Simon May, PMO, and Mr Rob Walker, Manager of Stakeholder Engagement. Each of these high-level CASA staff exercised due diligence in their deliberations and endorsed the OCVA. The present regime is utterly arrogant on this point alone.
- � Zealot: The definition of a zealot is someone who is fanatically passionate about a belief. The zealots in CASA treat the colour perception standard as if it were a sacred religious belief.
- � Insouciant: showing a casual lack of concern, in this instance, for the dire consequences of their beliefs on the career aspirations of many healthy actual and aspiring pilots. We are talking about a potential target population of perhaps as many as half a million citizens who, if they inquired, would be advised they cannot be or become career pilots.
- � sophistry: using clever but false arguments to deceive or confound. In this instance, CASA's (i.e. Kate Manderson's) assertion that "absence of evidence is not evidence of absence" is pure sophistry. It would have us believe that no evidence indicating safe performance by CVD pilots will ever lead them to conclude that CVD is not a safety risk.
- � BS: a polite shortening of a well-known Australian term meaning lies, rubbish, nonsense, etc., etc. The posts above give many instances of BS perpetrated by CASA. Everything about this "project" reeks of BS
- �Fraud: the fraudulent presentation on at least two occasions at aviation medical "scientific" meetings of an accident due purportedly to the pilot's colour vision defect by a senior medical staff member of the NZ CAA was a significant element in swaying the NZ CAA that there was a deep bias in their medical section. Complaints made to the Victorian and National organisers resulted in effectively no reprimand to the perpetrator. Here is the link to a report on this matter to the NZ CAA advisory panel on the topic: PMO review submission to CAA NZ
What we have now is an unholy mess. It takes us back to worse conditions and restrictions than in the 1970's. Dr Manderson and her deputy, Dr Hochberg, are true believers and have learnt nothing from the three AAT outcomes that ultimately led Director Carmody and Dr Simon May to adopt and implement the OCVA.
The purpose of the OCVA test was to satisfy a duly qualified examiner of airmen that a candidate for a medical certificate could identify the information needed to perform a pilot's duties safely. The adoption of the OCVA followed extensive investigation, consultation, and consideration on both sides of the Tasman. Both the CAA NZ and CASA directors had face-to-face meetings with each other and the entire industry. The Aviation Safety Advisory Panel (ASAP) supported implementing the OCVA unanimously.
A pass on the OCVA posed no threat of any description to the safety of air navigation, as it didn't qualify the candidate to perform any task involved in flying an aircraft. It made it possible to study, train and be tested in the same manner as a candidate with normal colour vision. Safe operation performance is a subject that medicos are not qualified to judge. This assessment falls in the domain of professional examiners of airmen.
Finally, I am not against medical standards. The safety implications of heart disease, hypertension, diabetes, and neurological diseases (e.g. epilepsy) are profound. A pilot having a fit, a heart attack, a stroke, or a hypoglycaemic episode is manifestly unlikely to be able to perform their duties as a pilot safely. Defective colour vision has no such dire consequences.
Last edited by Arthur Pape; 12th Nov 2023 at 04:09. Reason: an omission
The following 6 users liked this post by Arthur Pape:
If there were any substance to CASA AvMed’s concerns about the efficacy of the OCVA and compliance with ‘the international standard’, CASA would be calling loudly and courageously for:
- Cessation of commercial flights into Australia by crew medically certified by the NZCAA. Those crew include pilots certified to have met the colour perception criterion in the medical standard on the basis of the OCVA.
- Cessation of commercial flights of Australian aircraft into the NZ. The fare paying passengers on board those Australian aircraft are being exposed to risks arising from NZ aircraft in NZ with crew medically certified by the NZCAA.
Ditto commercial flights into Australia by crew medically certified by the FAA and commercial flights of Australian aircraft into the USA. The FAA certifies crew as having met the colour perception criterion in the medical standard on the basis of an operational test.
The dire safety consequences of CVD know no borders. CASA AvMed’s selfless leadership and commitment to the safety of air navigation surely demands a complete review of the way in which every country tests and certifies compliance with the colour perception standard, and a ‘banning’ of all commercial flights to and from all countries which do not test and certify in a way with which CASA Avmed is satisfied.
- Cessation of commercial flights into Australia by crew medically certified by the NZCAA. Those crew include pilots certified to have met the colour perception criterion in the medical standard on the basis of the OCVA.
- Cessation of commercial flights of Australian aircraft into the NZ. The fare paying passengers on board those Australian aircraft are being exposed to risks arising from NZ aircraft in NZ with crew medically certified by the NZCAA.
Ditto commercial flights into Australia by crew medically certified by the FAA and commercial flights of Australian aircraft into the USA. The FAA certifies crew as having met the colour perception criterion in the medical standard on the basis of an operational test.
The dire safety consequences of CVD know no borders. CASA AvMed’s selfless leadership and commitment to the safety of air navigation surely demands a complete review of the way in which every country tests and certifies compliance with the colour perception standard, and a ‘banning’ of all commercial flights to and from all countries which do not test and certify in a way with which CASA Avmed is satisfied.
Last edited by Clinton McKenzie; 9th Nov 2023 at 08:14.
The following 4 users liked this post by Clinton McKenzie:
Thread Starter
It's worth emphasising that although NZ CAA led the way with the introduction of the OCVA in 2019, this was not as a result of their AvMed unit. In fact, their PMO diametrically opposed any form of practical testing and according to CASA, the NZ AvMed unit still disagrees with the OCVA. Rather, we can be fortunate that the NZ CAA Director at the time and the Panel that was tasked with reviewing all the submissions and presentations from various experts (including medically and operationally) took an unbiased view and considered the facts:
NZ CAA - Report of the Colour Vision Deficiency General Direction Assessment Panel
As highlighted by Arthur, it's also no surprise then that the former CAA Director and the Panel chose to give such little weight to their PMO's opinions, particularly when considering his obvious bias against CVD pilots - as evidenced in presentations that he delivered to several aviation medicine scientific conferences.
PMO Review Submission to NZ CAA

Fortunately, the former CASA Director Shane Carmody also saw through this obvious bias from the AvMed zealots in both NZ and Australia at the time, when considering our position to adopt the OCVA here in 2020.
Lets hope that Ms Spence is also giving it the same consideration again currently.
NZ CAA - Report of the Colour Vision Deficiency General Direction Assessment Panel
15. ...In answer to a question regarding the reasoning behind the flight restrictions for a pilot who is CVD, the PMO answered that the �restrictions are historical�. This is a key issue for the Panel�s deliberations particularly in relation to the risk posed by a pilot with CVD, the different operational environments pilots operate in, and who should be determining restrictions to which a pilot is to operate.
16. The PMO also commented that he thought practical flight tests are unreliable. In the Panel�s opinion a flight examination has the same status as a medical examination in ensuring that a pilot is not a threat to the public and renewing their privilege to fly.
51. A substantial theme to emerge from the body of submissions is that the current PMO is biased and prejudiced against CVD pilots (25, 50, 41, 51, 54). The GAA, in particular, is vehement in its opposition to the current PMO and his views: �The PMO appears to be mounting a crusade for global bureaucratic conformity from his office in New Zealand, while conveniently overlooking his previously published, strong desire for evidence-based decisions in aeromedical matters� (50).
53. The CVA likewise state that the stricter testing and restrictions appear to be based on the personal views of the PMO, rather than on evidence. It notes �the continued suitability of the PMO for his role in regulating clinical test methods and medical restrictions for CVD pilots is questioned� (25). It is also argued by the CVA that the PMO�s presentation at the Australian Society of Aerospace Medical Annual Scientific meeting in Brisbane in 2014 was prejudicial, unbalanced, objectionable, and factually inaccurate.
128. There is no strong link between the office-based examination of CVD and real world realities. Under the proposed GD, the assessment of interferes with or likely to interfere with is ascertained from office-based assessments only. This assessment cannot be made from office-based tests only and can only be determined by an in-flight practical test. While both aviation medicine and flight operations specialists will need to be involved in the development of protocols for in-flight testing, only a flight examiner or flight instructor will be in a position to assess the ability of a pilot with a CVD condition to operate an aircraft safely. Thus the effect that a CVD condition will have on the ability of a pilot to safely exercise the privileges of a licence is a flight operations issue, not a medical issue.
As highlighted by Arthur, it's also no surprise then that the former CAA Director and the Panel chose to give such little weight to their PMO's opinions, particularly when considering his obvious bias against CVD pilots - as evidenced in presentations that he delivered to several aviation medicine scientific conferences.
PMO Review Submission to NZ CAA
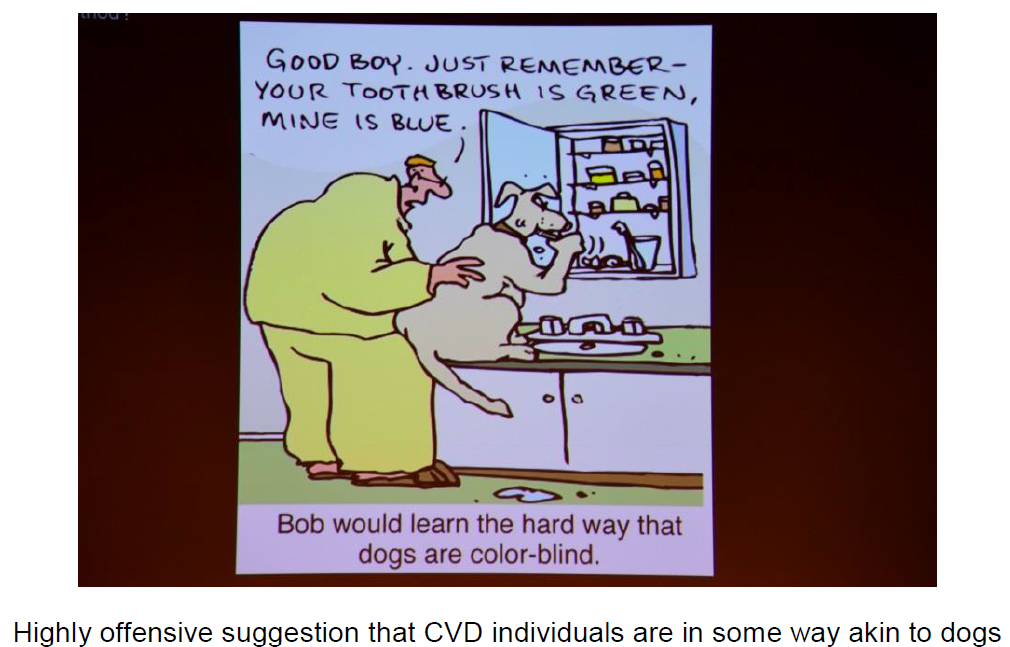
Despite the reasonably benign title, International Variation in the Assessment of Colour Vision Deficient Pilots, the presentation included a number of most disturbing slides including a plagiarized front page of The Times newspaper with a fabricated story which appears to be deliberately tailored to cast CVD pilots in a negative light.
Other slides containing false and misleading material in cartoon format were also displayed by the PMO, reflecting negatively on individuals with CVD. The public display of such humiliating and discriminatory material of this nature constitutes harassment of individuals with CVD.
The public display of similarly negative material about other minority groups would be unacceptable. It is particularly grave however that such material is being circulated publicly by the senior manager within CAA who is directly responsible for generating this GD, deciding the test and restrictions regimes that are applied to CVD pilots.
Aside from the use of misleading and falsified slides, the presentation contained factually incorrect text. It is not clear if this is due to a lack of knowledge on the part of the PMO or a deliberate intent to discredit CVD pilots.
Other slides containing false and misleading material in cartoon format were also displayed by the PMO, reflecting negatively on individuals with CVD. The public display of such humiliating and discriminatory material of this nature constitutes harassment of individuals with CVD.
The public display of similarly negative material about other minority groups would be unacceptable. It is particularly grave however that such material is being circulated publicly by the senior manager within CAA who is directly responsible for generating this GD, deciding the test and restrictions regimes that are applied to CVD pilots.
Aside from the use of misleading and falsified slides, the presentation contained factually incorrect text. It is not clear if this is due to a lack of knowledge on the part of the PMO or a deliberate intent to discredit CVD pilots.
Fortunately, the former CASA Director Shane Carmody also saw through this obvious bias from the AvMed zealots in both NZ and Australia at the time, when considering our position to adopt the OCVA here in 2020.
Lets hope that Ms Spence is also giving it the same consideration again currently.
The following 5 users liked this post by johnobr:
Thanks jonobr!
As I've stated over and over, I have been challenging this perfidious "standard" for over 40 years, and I want to make some further observations that I have made about the matter.
As I've stated over and over, I have been challenging this perfidious "standard" for over 40 years, and I want to make some further observations that I have made about the matter.
- The church of the TRUE BELIEVERS that colour recognition and naming are essential and indispensable in acquiring awareness of operationally safety-relevant information and has a worldwide membership. I know all the senior clergy, and they are: Doug Ivan (Ret Colonel USAF), Sally Evans (CAA UK PMO), Tony Evans (long-time PMO in ICAO), and Dougal Watson (now ex-PMO CAA NZ). Each of these has had roles in the AAT cases concerning the colour vision standard, opposing relaxation in any form.
- In NZ, Dr Watson trained his team well in matters of colour vision and then promptly encouraged their migrations at various times to become PMOs or deputy PMOs with CASA: Pooshan Navathe, Michael Drane, and Dr Tony Hochberg.
- They are encouraged and supported by senior members of the various faculties of optometry, who feed them just what they want to hear. I'll mention a few: Prof. Barry Cole (Victorian College of Optometry); Dr Alys Vingrys (also VCO and a disciple of Barry Cole); Prof John Barbur (City, University of London). Last but not least, there is Dr John Parkes, an occupational physician, who has one of the two CAD machines in Australia. The second CAD is in Sydney and operated by an ophthalmologist I have never met. Each individual, except the owner of the Sydney CAD, has also played roles in AAT colour vision proceedings, supporting the CASA position.
- Over the long years, I have collected and studied hundreds of works and documents derived from these people, including the many research projects commissioned by CASA and their overseas counterparts (NZ CAA, UK CAA and the FAA). Bringing them all into the spotlight would take more than a book. However, if and when they were relied upon as evidence in the AAT, I drew upon highly qualified research professionals to critically analyse the contents. These critics formed the backbone of witnesses for the appellants in the three AAT CVD hearings. I'll leave it there, but note that CASA did not fare well in the three proceedings.
- A common theme I have found used by proponents of strong CVD regulation is that the matter is "self-evident". That is, you just need to show where and how colour is used in the wider aviation environment (i.e. colour is used ubiquitously), and it is "self-evident" that an individual who cannot reliably recognise and name those colours is going to be "unsafe".
- CASA's medical staff like to parade "Evidence Pyramids" as evidence that their decisions are "evidence-based". Yet, in their professional conduct, they give scant regard to the truth or otherwise of what they present to the plebs. Ask, and I can provide many examples of this.
- Truth has been a victim throughout the colour vision discussion, which leads me to the question: where is the ethics in all of this? The medical profession is supposed to be bound by a set of fundamental ethics. Now, granted that Aviation Medicine is not fundamentally a branch of the profession entrusted with treating sick people, I'll avoid referencing the "Hippocratic Oath" (I'm tempted to misspell the word). But there are other ethics relating to avoiding bias in decision-making and detecting and declaring a conflict of interest, to mention just a couple. The history of the debate over the colour perception standard is replete with glaring instances of poorly hidden conflicts of interest. They are particularly poignant in the current atmosphere, where lies and conflicts of interest can be easily demonstrated about the CAD test. The CAD is an expensive tool to buy, and the inventor of the CAD, Prof John Barbur, also conducted the validation process (which is a misnomer). He is the director of a spin-off company that markets the CAD worldwide. This marketing initially claimed that the CAD was "aviation specific" and that it would be a reliable predictor of performance by a CVD pilot on the PAPI.
Dr John Parkes' should declare a conflict of interest in current deliberations, as he makes his living mainly from his CAD testing. But no, Dr Parkes is the chief instigator of the move to discredit the OCVA and replace it with something far more beneficial to himself (the ACVA as a supplement to his CAD testing). - Finally, I congratulate John O'Brien on the way he has stuck to his guns and fought hard for his phenomenal career while staying in the fight. I know hundreds of pilots whose careers were salvaged from CVD obscurity by the likes of John and who took the rewards and vanished. As you can see, we are once again faced with a dreadful enemy that is immune to sound evidence and probably will not willingly make the right decision: to give us back the OCVA and stop harassing good, honest people who want to be professional pilots.
I am, and I know John is, determined to achieve that outcome, even if it means going to the Federal Court.
Please consider contributing to the fight with financial support for the CVDPA.
There is a PayPal link on our website at WWW.cvdpa.com
Last edited by Arthur Pape; 10th Nov 2023 at 04:17.
The following 5 users liked this post by Arthur Pape:
I encourage every pilot, every aspiring pilot and anyone who cares about them to consider providing financial support for the CVDPA. Ultimately, the only thing that keeps the CVD zealots in check is exposure to the glare of external scrutiny of courts and tribunals.
You may not have CVD, but your turn will come when the zealots decide that your ‘condition’ justifies the sorts of egregious, intellectually dishonest nonsense through which pilots with CVD are put.
And an important disclaimer: Neither Dr Arthur Pape nor John O’Brien nor I make a red cent directly or indirectly from fighting the zealots. In contrast, there’s an entire industry making money out of CVD, and some of the people who make that money are invitees to CASA’s CVD echo chamber.
The truth will out, one way or the other, again, but we’re again up against ‘Brandolini’s Law’, commonly known as the ‘bull**** asymmetry’. That ‘Law’ says that the amount of energy and resources necessary to refute bull**** is an order of magnitude greater than the energy and resources it took to produce it.
Another analogy: The views of CVD zealots are like Paterson’s Curse or Salvation Jane, depending on where you live. They’re a noxious weed that propagates so easily and therefore take so much time and energy to get back under control.
You may not have CVD, but your turn will come when the zealots decide that your ‘condition’ justifies the sorts of egregious, intellectually dishonest nonsense through which pilots with CVD are put.
And an important disclaimer: Neither Dr Arthur Pape nor John O’Brien nor I make a red cent directly or indirectly from fighting the zealots. In contrast, there’s an entire industry making money out of CVD, and some of the people who make that money are invitees to CASA’s CVD echo chamber.
The truth will out, one way or the other, again, but we’re again up against ‘Brandolini’s Law’, commonly known as the ‘bull**** asymmetry’. That ‘Law’ says that the amount of energy and resources necessary to refute bull**** is an order of magnitude greater than the energy and resources it took to produce it.
Another analogy: The views of CVD zealots are like Paterson’s Curse or Salvation Jane, depending on where you live. They’re a noxious weed that propagates so easily and therefore take so much time and energy to get back under control.
The following 4 users liked this post by Clinton McKenzie:
CASA/AVMED modus operandi.
Quote Clinton McKenzie:-
� You may not have CVD, but your turn will come when the zealots decide that your �condition� justifies the sorts of egregious, intellectually dishonest nonsense through which pilots with CVD are put.�
I�ve been victim of exactly this type of behaviour from AVMED. For over twenty years I�ve been required to make an annual cardio test against the written advice of the conducting cardiologist on the basis that I have no symptoms that would call for such a test. AVMED�s illogical regime leading to expensive and time wasting examinations are repeated for hundreds if not thousands of pilots and will continue while its authority and mindset goes unchallenged. CASA�s current move, at glacial pace, toward a self declared medical is presented with so many restrictions it will make the proposal barely useful only for a small percentage of private pilots. Again the same thinking that�s confounding the CVD pilots.
We all need to support the CVD organisation, including with our donations.
� You may not have CVD, but your turn will come when the zealots decide that your �condition� justifies the sorts of egregious, intellectually dishonest nonsense through which pilots with CVD are put.�
I�ve been victim of exactly this type of behaviour from AVMED. For over twenty years I�ve been required to make an annual cardio test against the written advice of the conducting cardiologist on the basis that I have no symptoms that would call for such a test. AVMED�s illogical regime leading to expensive and time wasting examinations are repeated for hundreds if not thousands of pilots and will continue while its authority and mindset goes unchallenged. CASA�s current move, at glacial pace, toward a self declared medical is presented with so many restrictions it will make the proposal barely useful only for a small percentage of private pilots. Again the same thinking that�s confounding the CVD pilots.
We all need to support the CVD organisation, including with our donations.
The following 3 users liked this post by Sandy Reith:
Once again CASA AvMed sticks their head into a situation that was previously settled. Not a single person on earth would debate the fact that doctors can diagnose a Colour Vision Defect. This is where their knowledge on Colour Vision ends. They have not a clue on the first thing about how colour vision affects safe aviation. This should be left to flight crew licensing, real pilots not make believe pilots.
Seeing the above slides reminded me of a time where CASA AvMed thought it appropriate to send my employer an email saying that he employed a CVD pilot and he should consider the safety of that decision. This absolutely abhorrent torrent of attacks from CASA on a previously settled issue is at best a waste of tax payer money and at worst it's outright bullying and harassment of air crew. When I spoke on the phone to Tony Hochberg about what would happen to my medical as a result of this new "policy" I was given no answer and was told it would be on a "case by case basis". As someone with circa 5,000 hours this is lunacy.
This case has been fought again and again, and not once has CASA ever won a decision on it outside of their own dictatorship. When will the madness end.
Seeing the above slides reminded me of a time where CASA AvMed thought it appropriate to send my employer an email saying that he employed a CVD pilot and he should consider the safety of that decision. This absolutely abhorrent torrent of attacks from CASA on a previously settled issue is at best a waste of tax payer money and at worst it's outright bullying and harassment of air crew. When I spoke on the phone to Tony Hochberg about what would happen to my medical as a result of this new "policy" I was given no answer and was told it would be on a "case by case basis". As someone with circa 5,000 hours this is lunacy.
This case has been fought again and again, and not once has CASA ever won a decision on it outside of their own dictatorship. When will the madness end.
The following 4 users liked this post by papakurapilot:
� When will the madness end?�
The short answer is it won�t end until and unless there�s political willpower to recognise the abject failure of the governance model.
That is the creation of an independent Commonwealth corporation to oversee and administer our civil aviation. A make work salary factory that has in reality a primary responsibility to itself.
It was 1988 when Labor Minister Gareth Evans decided to rid himself of direct responsibility for aviation with the predictable consequences we see writ large today.
The action completely disregarded a fundamental principle of the Westminster system, that is that responsibility lies with a Minister for the various arms of government administration. Unfortunately not one Minister or government of either stripe has had the intestinal fortitude to correct this wasteful and industry debilitating situation.
Much as we love to blame our MPs, few bother to actually engage with our elected representatives, and this is our responsibility if we want our democracy to improve.
That is the creation of an independent Commonwealth corporation to oversee and administer our civil aviation. A make work salary factory that has in reality a primary responsibility to itself.
It was 1988 when Labor Minister Gareth Evans decided to rid himself of direct responsibility for aviation with the predictable consequences we see writ large today.
The action completely disregarded a fundamental principle of the Westminster system, that is that responsibility lies with a Minister for the various arms of government administration. Unfortunately not one Minister or government of either stripe has had the intestinal fortitude to correct this wasteful and industry debilitating situation.
Much as we love to blame our MPs, few bother to actually engage with our elected representatives, and this is our responsibility if we want our democracy to improve.
The following users liked this post:
Some further ‘highlights’ from the documents disclosed under FOI and some comments arising from the content of the posts above.
When will the madness end?
When will the madness end? When some proper governance is applied again to CASA AvMed. As a consequence of inadequate governance, combined with how stressful and costly it is to take them on, CASA AvMed reckons the medical standards can practicably be whatever they reckon the standards should be, rather than what the law says the standards are. If the people paid to secure compliance of these zealots with proper governance requirements – Ms Spence and the CASA Board – won’t do it, it’s left once again to individuals to fight them in the courts and tribunals.
The awful safety risks and the change in name
The CASA AvMed echo chamber papers released under FOI list 3 ‘safety concerns’, the third of which is:
Newsflash, zealots: A person who has ‘passed Farnsworth’ in accordance with either CASR 67.150(6)(b) or CASR 67.155(6)(b) has demonstrated compliance with the colour perception criterion of the corresponding medical standard in Part 67. Full stop.
It should not matter whether the CVD zealots have an attack of the vapours about that. If they understood their duties as public officials administering the law they would understand that their personal opinions as to what constitutes compliance with the colour perception criterion are irrelevant. Unfortunately, they don’t have proper governance around them and they’ve been left to their own devices to implement the system their religion dictates, despite the law. These are public officials in government agency in the 21st century.
Someone who has ‘failed OCVA’ may be plain incompetent. Have the zealots been running a control experiment requiring pilots with ‘normal’ vision to undertake the OCVA to confirm that no pilot with ‘normal’ vision will ever fail the OCVA? (And by the way: the person who failed the OCVA puts the lie to the suggestion that no one has failed the OCVA.) I’ve never passed the Farnsworth test, the CAD or the OCVA.
And in the case of the OCVA “which was incomplete”, whose fault is that? The candidate just did whatever the candidate was told by the examiner, for as long as the candidate was told to do it by examiner. Maybe AvMed should have a chat with the examiner who did not administer a ‘complete’ OCVA?
I initially attributed the change in name from OCVA to ACVA to a manifestation of the self-appointed leadership of the Australian zealots. But then I was reminded, by the discussion above, that it’s another manifestation of the zealots’ obsession with CVD being a medical issue not an operational issue. I’ve seen the proposed ACVA described in CASA correspondence as a “medical flight test”.
The zealots’ religion simply refuses to accept that the ability to interpret information from an environment with different colours is an operational assessment, because being a doctor does not qualify someone to test whether a pilot is interpreting information adequately. And the zealots can hold their breath and stamp their little feet until their faces turn blue, but the applicable CASR says – remember that mere bagatelle the law – that the third tier test must ‘simulate an operational situation’.
More from the CASA AvMed echo chamber papers released under FOI. And this is the gist of the ‘safety’ issue arising from CVD, in the zealots’ religion:
And there you have it: Twofold nonsense.
The first nonsense is that in the aviation environment the colour of something is the sole cue and sole source of important information. The second and most palpable nonsense is that pilots with CVD are never put through any stressful, emergency situations and tested against objective standards of performance.
You couldn’t make this stuff up. It would be laughable if so many people’s careers and career aspirations weren't on the line.
When the zealots can specify the number of milliseconds that marks the boundary between ‘safe’ and ‘unsafe’ recognition times for each piece of information in the operational aviation environment, they can get those numbers put in the MOS and get every candidate tested against those numbers. At the moment, their religion dictates that it ‘must’ take pilots with CVD ‘longer’ to interpret information and therefore they must be ‘less safe’ than pilots without CVD. Just like female pilots must be less safe than male pilots because female pilots can’t lift as much weight as quickly as males and physical strength can become the determining factor between safety and an accident in an emergency.
Compliance with ICAO
As was so eloquently pointed out earlier – with reference to the number of pages of differences filed by Australia – the claimed ICAO compliance issue is a smokescreen. As CASA is so quick to point out – correctly – when it is convenient for CASA: There is only one obligation on member states to the Chicago Convention, and that is to notify of differences from SARPS. That’s why Australia has ‘filed’ so many ‘differences’. But for the zealots on the CVD crusade, their interpretation of the Convention provisions on colour perception is immutable, holy writ. Any difference from that interpretation is, by definition, unsafe. (Yet strangely, as I pointed out earlier, CASA isn’t calling loudly and courageously for the ‘banning’ of anything that would expose us to the risks arising from those dangerous CVD pilots from the NZ or the USA, for example.)
Lying by omission
That oft-repeated statement by various CASA people, from various CEOs down, about the number of medical ‘approvals’ or certificates granted and refused falls within the scope of what I define as a “lie by omission”: Stating a fact but omitting another important fact in order deliberately to foster a misconception.
An ordinary member of the public would assume that if CASA has issued a person a medical certificate in fact, that person has nothing to whinge about. CASA issues (a claimed and oddly consistently round figure over years of) 25,000 medical ‘approvals’ or certificates (the word varies depending on who’s speaking) and knocks back fewer than 100. How could the holder of one of these approvals/certificates possibly have any ground to complain?
Of course, us guinea pigs in the process know the whole truth about the costly and dangerous tests imposed by AvMed which tests qualified medical professionals say are unnecessary, and the conditions imposed by AvMed which effectively destroy – among other things – careers and career aspirations.
The only way in which I am able to give Ms Spence the benefit of the doubt is to assume that she’s completely ignorant as to what medical certificate applicants are put through and what ends up on their certificates.
“We issued driver’s licences to all those aspiring race car drivers with CVD!” (Forgot to mention: all of those licences are subject to the condition that the holder never exceed 60kph.)
Intellectual dishonesty
I was first struck by the extent of the intellectual dishonesty of the CVD zealots when I read some of the stuff produced by Dougal Watson. I could not believe that someone so obviously blinded by prejudice and his consequentially flawed reasoning could be taken seriously in any forum of qualified academics and medical professionals. I literally could not believe it. Then through discussions with Arthur Pape I came to realise that these ‘forums’ are actually echo chambers in which the CVD zealots perform their religious rites.
Then I read the NTSB report on the Tallahassee B727 which landed short in 2002. That report is referred to and partially quoted at Annex C of the CASA echo chamber papers released under FOI. Conclusion 13 of 16 conclusions is that: “The first officer suffered from a severe color vision deficiency that made it difficult for him to correctly identify the color of the precision approach path indicator signal during the below-glidepath, nighttime, visual approach to runway 9 at Tallahassee Regional Airport.” I came to that report with an open mind and the presumption that it would be the product of cold, hard analysis by disinterested professionals.
I then read the report.
I commend the report to anyone who hasn't read it. I’ll cherry pick bits below, but everyone should read the entire report and form their own views. I would particularly like to hear from people who, first, do not have any direct or indirect interest in CVD and, secondly, consider that CVD had any causal connection with the accident.
So pause there and note: 3 pilots on board.
So pause there and note: The pilot with CVD was pilot flying.
So pause there and note the local time and the meteorological conditions - in particular the temp and dew point.
Recall that the ‘flight engineer’ is also a pilot.
The flight continues, with discussions about what runway would be used etc. Ultimately they decide on 09. Then…
So note: The captain (no CVD) effectively told the first officer (with CVD) that the GPWS warning was nothing to worry about.
It's about here that I started to get an inkling of the intellectual dishonesty that infects this report:
Note the words “would have”. Not “should have” or “would probably have”, but an expression of certainty: “would have”. The only people qualified to give first-hand evidence of what was being displayed at the time of the approach of the accident aircraft are the people who were looking at what was being displayed at that time.
PAPI used to have a latent defect. But it became a patent defect decades ago. The patent defect is that in some atmospheric conditions PAPI does not do what it should do. “The Safety Board’s airplane” did not fly the approach at the same local time in the same weather conditions as the B727 involved in the accident did.
I’ll jump forward a bit in the report to highlight these two tidbits:
Presumably NATCA just made it up. Presumably posters on this forum who report observing ‘four pinks’ on Australian PAPIs are making it up too.
Strangely, though, the report also says:
Go figure. Why would that rewiring be necessary if there was never any contamination of the TLH PAPI lights just before dawn with the reported temp and dew point being the same?
But back to what the report says about the accident sequence:
When I read that, as someone without CVD and no direct or indirect pecuniary or other interest in CVD testing, I conclude that, to the extent - if any - that colour vision had any causal connection with the accident, it’s ‘normal’ colour vision that is the problem. Or maybe pilots with ‘normal’ colour vision, like the captain and flight engineer in this case, are more prone to lie about what they saw. Maybe the NACTA people who stated that there was a “high level of physical particle contamination” on the runway 9 PAPI boxes at TLH were liars, too.
And then you find out that the first officer also spent 16 years in the USN.
And then there’s all this analysis of military colour vision testing. And on it goes.
But when you scratch the surface of the cited authorities, you see the names of the ‘usual suspects’. The adherents to the religion. The same people in the same echo chamber.
Please read it for yourself and let me know what you think.
When will the madness end?
When will the madness end? When some proper governance is applied again to CASA AvMed. As a consequence of inadequate governance, combined with how stressful and costly it is to take them on, CASA AvMed reckons the medical standards can practicably be whatever they reckon the standards should be, rather than what the law says the standards are. If the people paid to secure compliance of these zealots with proper governance requirements – Ms Spence and the CASA Board – won’t do it, it’s left once again to individuals to fight them in the courts and tribunals.
The awful safety risks and the change in name
The CASA AvMed echo chamber papers released under FOI list 3 ‘safety concerns’, the third of which is:
3. CVD cases recently cleared of all colour vision endorsements include:
- Cl 1 pilot who failed OCVA but passed Farnsworth - all CVD conditions/ restrictions removed
- Cl 1 pilot who fail PAPI but passed Farnsworth - all CVD conditions/ restrictions removed
- Cl 1 pilot with 0.5 hours flight experience severe CVD – passed OCVA which was incomplete
- Cl 1 pilot who failed OCVA but passed Farnsworth - all CVD conditions/ restrictions removed
- Cl 1 pilot who fail PAPI but passed Farnsworth - all CVD conditions/ restrictions removed
- Cl 1 pilot with 0.5 hours flight experience severe CVD – passed OCVA which was incomplete
It should not matter whether the CVD zealots have an attack of the vapours about that. If they understood their duties as public officials administering the law they would understand that their personal opinions as to what constitutes compliance with the colour perception criterion are irrelevant. Unfortunately, they don’t have proper governance around them and they’ve been left to their own devices to implement the system their religion dictates, despite the law. These are public officials in government agency in the 21st century.
Someone who has ‘failed OCVA’ may be plain incompetent. Have the zealots been running a control experiment requiring pilots with ‘normal’ vision to undertake the OCVA to confirm that no pilot with ‘normal’ vision will ever fail the OCVA? (And by the way: the person who failed the OCVA puts the lie to the suggestion that no one has failed the OCVA.) I’ve never passed the Farnsworth test, the CAD or the OCVA.
And in the case of the OCVA “which was incomplete”, whose fault is that? The candidate just did whatever the candidate was told by the examiner, for as long as the candidate was told to do it by examiner. Maybe AvMed should have a chat with the examiner who did not administer a ‘complete’ OCVA?
I initially attributed the change in name from OCVA to ACVA to a manifestation of the self-appointed leadership of the Australian zealots. But then I was reminded, by the discussion above, that it’s another manifestation of the zealots’ obsession with CVD being a medical issue not an operational issue. I’ve seen the proposed ACVA described in CASA correspondence as a “medical flight test”.
The zealots’ religion simply refuses to accept that the ability to interpret information from an environment with different colours is an operational assessment, because being a doctor does not qualify someone to test whether a pilot is interpreting information adequately. And the zealots can hold their breath and stamp their little feet until their faces turn blue, but the applicable CASR says – remember that mere bagatelle the law – that the third tier test must ‘simulate an operational situation’.
More from the CASA AvMed echo chamber papers released under FOI. And this is the gist of the ‘safety’ issue arising from CVD, in the zealots’ religion:
[C]olour dependent cues are most important in critical phases of flight, add to this an emergency on-board, with heightened stress levels, the reaction time can become the determining factor between safety and accident.
The first nonsense is that in the aviation environment the colour of something is the sole cue and sole source of important information. The second and most palpable nonsense is that pilots with CVD are never put through any stressful, emergency situations and tested against objective standards of performance.
You couldn’t make this stuff up. It would be laughable if so many people’s careers and career aspirations weren't on the line.
When the zealots can specify the number of milliseconds that marks the boundary between ‘safe’ and ‘unsafe’ recognition times for each piece of information in the operational aviation environment, they can get those numbers put in the MOS and get every candidate tested against those numbers. At the moment, their religion dictates that it ‘must’ take pilots with CVD ‘longer’ to interpret information and therefore they must be ‘less safe’ than pilots without CVD. Just like female pilots must be less safe than male pilots because female pilots can’t lift as much weight as quickly as males and physical strength can become the determining factor between safety and an accident in an emergency.
Compliance with ICAO
As was so eloquently pointed out earlier – with reference to the number of pages of differences filed by Australia – the claimed ICAO compliance issue is a smokescreen. As CASA is so quick to point out – correctly – when it is convenient for CASA: There is only one obligation on member states to the Chicago Convention, and that is to notify of differences from SARPS. That’s why Australia has ‘filed’ so many ‘differences’. But for the zealots on the CVD crusade, their interpretation of the Convention provisions on colour perception is immutable, holy writ. Any difference from that interpretation is, by definition, unsafe. (Yet strangely, as I pointed out earlier, CASA isn’t calling loudly and courageously for the ‘banning’ of anything that would expose us to the risks arising from those dangerous CVD pilots from the NZ or the USA, for example.)
Lying by omission
That oft-repeated statement by various CASA people, from various CEOs down, about the number of medical ‘approvals’ or certificates granted and refused falls within the scope of what I define as a “lie by omission”: Stating a fact but omitting another important fact in order deliberately to foster a misconception.
An ordinary member of the public would assume that if CASA has issued a person a medical certificate in fact, that person has nothing to whinge about. CASA issues (a claimed and oddly consistently round figure over years of) 25,000 medical ‘approvals’ or certificates (the word varies depending on who’s speaking) and knocks back fewer than 100. How could the holder of one of these approvals/certificates possibly have any ground to complain?
Of course, us guinea pigs in the process know the whole truth about the costly and dangerous tests imposed by AvMed which tests qualified medical professionals say are unnecessary, and the conditions imposed by AvMed which effectively destroy – among other things – careers and career aspirations.
The only way in which I am able to give Ms Spence the benefit of the doubt is to assume that she’s completely ignorant as to what medical certificate applicants are put through and what ends up on their certificates.
“We issued driver’s licences to all those aspiring race car drivers with CVD!” (Forgot to mention: all of those licences are subject to the condition that the holder never exceed 60kph.)
Intellectual dishonesty
I was first struck by the extent of the intellectual dishonesty of the CVD zealots when I read some of the stuff produced by Dougal Watson. I could not believe that someone so obviously blinded by prejudice and his consequentially flawed reasoning could be taken seriously in any forum of qualified academics and medical professionals. I literally could not believe it. Then through discussions with Arthur Pape I came to realise that these ‘forums’ are actually echo chambers in which the CVD zealots perform their religious rites.
Then I read the NTSB report on the Tallahassee B727 which landed short in 2002. That report is referred to and partially quoted at Annex C of the CASA echo chamber papers released under FOI. Conclusion 13 of 16 conclusions is that: “The first officer suffered from a severe color vision deficiency that made it difficult for him to correctly identify the color of the precision approach path indicator signal during the below-glidepath, nighttime, visual approach to runway 9 at Tallahassee Regional Airport.” I came to that report with an open mind and the presumption that it would be the product of cold, hard analysis by disinterested professionals.
I then read the report.
I commend the report to anyone who hasn't read it. I’ll cherry pick bits below, but everyone should read the entire report and form their own views. I would particularly like to hear from people who, first, do not have any direct or indirect interest in CVD and, secondly, consider that CVD had any causal connection with the accident.
The accident flight crew consisted of three reserve FedEx pilots. The accident flight was the first time all three crewmembers had flown together; however, the captain and flight engineer had flown together once previously.
The first officer was the flying pilot, while the captain performed the non-flying pilot duties for the accident flight.
According to the CVR transcript, about 0511, the flight engineer received the TLH weather information from the Gainesville Flight Service Station, which indicated: scattered clouds at 100 feet, 18,000 feet, and 25,000 feet; wind from 120� at 5 knots; visibility 9 statute miles; temperature and dew point 22� C (Celsius); and altimeter setting 30.10 inches of mercury (Hg)
The flight engineer then briefed the captain and first officer regarding parking at TLH and, in accordance with company procedures, advised them that FedEx considered TLH a moderate controlled flight into terrain (CFIT) risk.
The flight continues, with discussions about what runway would be used etc. Ultimately they decide on 09. Then…
About 0530:32, the CVR recorded sounds similar to a microphone being keyed five times within about 1.3 seconds. About 7 seconds later, the captain radioed “Tallahassee uh FedEx fourteen seventy eight uh extended uh left base leg for runway nine.” The first officer indicated that he thought he saw the runway about 0530:56; he called for “flaps 2” about 0531:10 and “flaps 5” about 12 seconds later. About 0532:34, the first officer stated, “I hope I’m lookin’ in the right spot here.” The captain responded, “see that group of bright lights kinda to the south down there and you see the beacon in the middle of it? right over there you’re kinda on about ten mile left base or so.” The first officer then indicated that he had been “�looking at the wrong flashin’ light.”
About 0533:05, the first officer repeated, “I was lookin ‘at the wrong light,” and the captain responded, “yeah okay, yeah.” The first officer added, “yeah, with the direction I took, we coulda used [runway] 27, eh?”, and the captain responded, “yeah, it dudn’t matter. Yeah, it’s about ten miles south of the VOR.”
About 0534:11, the captain stated, “I guess the lights came on, if not I’ll click ‘em again here when we get a little closer.” About 20 seconds later, the CVR recorded a sound similar to a microphone being keyed five times within about 1.5 seconds, and, at 0534:35, the captain said, “there we go.” The first officer requested “flaps 15” about 0535:24. About 0535:31, the first officer stated, “gear down, before landing check;” about 2 seconds later, the CVR recorded a sound similar to the landing gear handle being operated followed by a sound similar to the nose gear door opening.
….
About 0536:20, the first officer said, “sorry about that. I was linin’ up on that papermill or something.” As the first officer started speaking, (at 0536:20.2), the CVR recorded the ground proximity warning system (GPWS) announce that the airplane passed through 1,000 feet above ground level (agl). About 0536:23, the captain said, “that’s all right, no problem.”
About 0533:05, the first officer repeated, “I was lookin ‘at the wrong light,” and the captain responded, “yeah okay, yeah.” The first officer added, “yeah, with the direction I took, we coulda used [runway] 27, eh?”, and the captain responded, “yeah, it dudn’t matter. Yeah, it’s about ten miles south of the VOR.”
About 0534:11, the captain stated, “I guess the lights came on, if not I’ll click ‘em again here when we get a little closer.” About 20 seconds later, the CVR recorded a sound similar to a microphone being keyed five times within about 1.5 seconds, and, at 0534:35, the captain said, “there we go.” The first officer requested “flaps 15” about 0535:24. About 0535:31, the first officer stated, “gear down, before landing check;” about 2 seconds later, the CVR recorded a sound similar to the landing gear handle being operated followed by a sound similar to the nose gear door opening.
….
About 0536:20, the first officer said, “sorry about that. I was linin’ up on that papermill or something.” As the first officer started speaking, (at 0536:20.2), the CVR recorded the ground proximity warning system (GPWS) announce that the airplane passed through 1,000 feet above ground level (agl). About 0536:23, the captain said, “that’s all right, no problem.”
It's about here that I started to get an inkling of the intellectual dishonesty that infects this report:
About 0536:37, the airplane was slightly more than 2.5 nautical miles (nm) from the airport and was transitioning from an angled base-to-final leg to line up with the runway. The Safety Board’s airplane performance study indicated that, about this time, the PAPI would have been displaying one white light and three red lights when viewed from the cockpit. About 0536:40, the PAPI display would have shown four red lights.
PAPI used to have a latent defect. But it became a patent defect decades ago. The patent defect is that in some atmospheric conditions PAPI does not do what it should do. “The Safety Board’s airplane” did not fly the approach at the same local time in the same weather conditions as the B727 involved in the accident did.
I’ll jump forward a bit in the report to highlight these two tidbits:
The Safety Board notes that the National Air Traffic Controllers Association (NATCA) submission on this accident stated that there was a “high level of physical particle contamination” on the runway 9 PAPI boxes at TLH. However, investigators who examined the PAPI boxes during the on-scene investigation (including the NATCA representative and other members of the investigative team) noted no such contamination, and the investigation developed no evidence to support this contention.
Strangely, though, the report also says:
On December 12, 2002, the FAA issued CertAlert Number 02-08, “PAPI Operation” which advised that 14 CFR Part 139-certificated airport operators should “rewire pilot controlled PAPI systems to make them operate continuously in order to preclude environmental contamination of the lenses.” The TLH PAPI lights were subsequently rewired in accordance with the CertAlert.
But back to what the report says about the accident sequence:
During postaccident interviews, all three crewmembers described a normal flight until the last seconds of the approach. The captain stated that the airplane was established on final as it descended through about 800 feet. He stated that during the approach, he observed “white pink, going to white red” on the PAPI and that, as the airplane descended, “we started picking up a few little wispy, I want to say clouds or mist, but it didn’t obscure the airport.” The captain stated that his last recollection was of a “white red” PAPI indication, then “we started feeling a little bumping, and the rest of it I don’t recall.” The captain stated that the last thing he remembered about the approach was that “everything visually looked normal, based on the runway and that’s why I was somewhat shocked when I felt the thumping”.
The first officer stated the following about the approach:
“Everything was running exactly the way it was supposed to run. When we got down closer to the field and we had slowed down and the field was in sight and the wind was still prevailing down runway nine. And that’s when I mentioned should we go ahead and land on runway nine, since that’s where the wind is. [The captain] said okay, that’s fine. We were kinda lined up that direction anyway. And the speed was well within parameters Got the nose pointed to the airport, started slowing down, started dirtying up rolled out on the centerline on the PAPI I remember specifically adding a touch of power because I recall rolling out on centerline but 2 knots slow and a hair under the bug that’s the last I can remember I have no memory of the remainder of the flight.”
The first officer stated that when he first saw the PAPI lights, they indicated white next to red, showing that the airplane was on the glidepath. When investigators asked him to describe the PAPI system, the first officer described two white lights with two red lights next to each other. The first officer said that he would not have considered landing on runway 9 if it did not have the PAPI light guidance. He went on to state, “from the time I rolled out, I saw that I was on glideslope, added that power for the 2 knots, and it never changed. After that, since I have no memory of the remainder of the flight...I don’t know where the rest of the flight went.” When asked about power settings, the first officer told investigators that fuel flow for a normal visual approach would be 3,000 to 3,500 pounds per hour (pph) at 500 feet.
The flight engineer told investigators that he first saw the airport about the same time the first officer remarked that he had the runway in sight, when the airplane was on a modified left base leg for runway 9. The flight engineer stated that, when he first saw the runway, he observed a white, a pink, and two red lights on the runway’s four-light PAPI system. He further stated that, throughout the approach, he was scanning his instruments and looking outside for other air traffic and that, as they neared the runway, they could see the runway lights “plain as day, including the PAPI.” He stated that the visibility was good during their approach and indicated that he did not observe any of the low, scattered clouds that were reported in the TLH weather observation.
The first officer stated the following about the approach:
“Everything was running exactly the way it was supposed to run. When we got down closer to the field and we had slowed down and the field was in sight and the wind was still prevailing down runway nine. And that’s when I mentioned should we go ahead and land on runway nine, since that’s where the wind is. [The captain] said okay, that’s fine. We were kinda lined up that direction anyway. And the speed was well within parameters Got the nose pointed to the airport, started slowing down, started dirtying up rolled out on the centerline on the PAPI I remember specifically adding a touch of power because I recall rolling out on centerline but 2 knots slow and a hair under the bug that’s the last I can remember I have no memory of the remainder of the flight.”
The first officer stated that when he first saw the PAPI lights, they indicated white next to red, showing that the airplane was on the glidepath. When investigators asked him to describe the PAPI system, the first officer described two white lights with two red lights next to each other. The first officer said that he would not have considered landing on runway 9 if it did not have the PAPI light guidance. He went on to state, “from the time I rolled out, I saw that I was on glideslope, added that power for the 2 knots, and it never changed. After that, since I have no memory of the remainder of the flight...I don’t know where the rest of the flight went.” When asked about power settings, the first officer told investigators that fuel flow for a normal visual approach would be 3,000 to 3,500 pounds per hour (pph) at 500 feet.
The flight engineer told investigators that he first saw the airport about the same time the first officer remarked that he had the runway in sight, when the airplane was on a modified left base leg for runway 9. The flight engineer stated that, when he first saw the runway, he observed a white, a pink, and two red lights on the runway’s four-light PAPI system. He further stated that, throughout the approach, he was scanning his instruments and looking outside for other air traffic and that, as they neared the runway, they could see the runway lights “plain as day, including the PAPI.” He stated that the visibility was good during their approach and indicated that he did not observe any of the low, scattered clouds that were reported in the TLH weather observation.
And then you find out that the first officer also spent 16 years in the USN.
And then there’s all this analysis of military colour vision testing. And on it goes.
But when you scratch the surface of the cited authorities, you see the names of the ‘usual suspects’. The adherents to the religion. The same people in the same echo chamber.
Please read it for yourself and let me know what you think.
Last edited by Clinton McKenzie; 12th Nov 2023 at 09:19.
The following 4 users liked this post by Clinton McKenzie:
SITREP will be broadcast at 2pm (EADT) this Thursday (16 Nov 23):
Tallahassee B727
Anyone who has followed the some forty year saga of colour vision impairment in pilots won�t need to be persuaded.
Just as it appears that the sun orbits Earth so it is necessary (not) that all pilots must have exemplary colour vision in order to accomplish their flight duties in a safe and efficient manner.
In my view the lessor colour perception of around one in ten men should not be called �deficient� because it�s so common as to be normal.
Whilst we do battle with The Empire in Australia, more correctly that we continue to be steamrolled and frightened into submission, we often look longingly to the US of A where their system is light years in advance of ours. But occasionally their �Empire� has a slippage, some of their crew, hopefully a tiny minority, go the path of CASA.
One memorable example concerned the remarkable Bob Hoover who lost his USA medical because the FAA decided his red nose indicated he was drinking too much. He came to Australia and performed at the Avalon Airshow, having passed our medical.
It was my privilege to watch his incredible aerobatic flying routine which terminated after his rollout off the sealed strip onto the grass, both engines feathered, and he braked to a stop placing his left hand spinner in the upraised palm of the announcer�s hand.
He exited the Shrike to be interviewed by the said announcer, yours truly hanging by the fence just a few meters away, and he forcefully announced that he was grateful to Australia and that he could now fly anywhere in the world except in the USA because of an intransigent FAA medical officer. Not long after his return to the USA he regained his medical, they were shamed into restoring his flying status.
Asked to describe how it is to fly his airshow routine, he said in his Southern drawl, �well it�s like milking a mouse with big heavy gloves on.�
But that�s another story, the colour vision saga continues because the make work salary factory must keep on finding new and complex reasons for its existence, the truth or commonsense is too obtuse to the mind when power and money are the drivers.
Just as it appears that the sun orbits Earth so it is necessary (not) that all pilots must have exemplary colour vision in order to accomplish their flight duties in a safe and efficient manner.
In my view the lessor colour perception of around one in ten men should not be called �deficient� because it�s so common as to be normal.
Whilst we do battle with The Empire in Australia, more correctly that we continue to be steamrolled and frightened into submission, we often look longingly to the US of A where their system is light years in advance of ours. But occasionally their �Empire� has a slippage, some of their crew, hopefully a tiny minority, go the path of CASA.
One memorable example concerned the remarkable Bob Hoover who lost his USA medical because the FAA decided his red nose indicated he was drinking too much. He came to Australia and performed at the Avalon Airshow, having passed our medical.
It was my privilege to watch his incredible aerobatic flying routine which terminated after his rollout off the sealed strip onto the grass, both engines feathered, and he braked to a stop placing his left hand spinner in the upraised palm of the announcer�s hand.
He exited the Shrike to be interviewed by the said announcer, yours truly hanging by the fence just a few meters away, and he forcefully announced that he was grateful to Australia and that he could now fly anywhere in the world except in the USA because of an intransigent FAA medical officer. Not long after his return to the USA he regained his medical, they were shamed into restoring his flying status.
Asked to describe how it is to fly his airshow routine, he said in his Southern drawl, �well it�s like milking a mouse with big heavy gloves on.�
But that�s another story, the colour vision saga continues because the make work salary factory must keep on finding new and complex reasons for its existence, the truth or commonsense is too obtuse to the mind when power and money are the drivers.
The following 3 users liked this post by Sandy Reith:
Underlying science
Following Clinton's brilliant post, I thought I'd inform the debate further with the following links"Clark and Gordon Hazards of Colour Coding in Visual Approach Slope Indicators
This link is to a document, published by the Australian Defence Research Laboratories, which very clearly describes the inherent risks of contamination of the PAPI code, based on red/white discrimination, resulting in the distortion of the signal and ultimately, when it fails, it fails "UNSAFE".
When you've read this, and compared it with the NTSB report, it will be manifestlyclear that the crash was entirely due to a "fail unsafe" scenario with the Tallahassee RWY 9 PAPI.
The second link is to a paper, co-authored by myself and Boris Crassini, analyzing the dilemma inherent in the crash investigation, and proposing an alternative explanation (to that reached by the NTSB) of the crash. The Puzzle of the Crash of Fedex Flight 1478: Implications for Colour Vision Standards in Aviation
:Thank you Clinton for bringing on this discussion.
Do note that the Clark and Gordon document does predict that CVD pilots may have difficulties identifying the PAPI code in certain circumstances, a conclusion I don't have any problem accepting.
To me the Fedex crash circumstances were a perfect fit for the predictions made by Clark and Gordon
This link is to a document, published by the Australian Defence Research Laboratories, which very clearly describes the inherent risks of contamination of the PAPI code, based on red/white discrimination, resulting in the distortion of the signal and ultimately, when it fails, it fails "UNSAFE".
When you've read this, and compared it with the NTSB report, it will be manifestlyclear that the crash was entirely due to a "fail unsafe" scenario with the Tallahassee RWY 9 PAPI.
The second link is to a paper, co-authored by myself and Boris Crassini, analyzing the dilemma inherent in the crash investigation, and proposing an alternative explanation (to that reached by the NTSB) of the crash. The Puzzle of the Crash of Fedex Flight 1478: Implications for Colour Vision Standards in Aviation
:Thank you Clinton for bringing on this discussion.
Do note that the Clark and Gordon document does predict that CVD pilots may have difficulties identifying the PAPI code in certain circumstances, a conclusion I don't have any problem accepting.
To me the Fedex crash circumstances were a perfect fit for the predictions made by Clark and Gordon
Last edited by Arthur Pape; 16th Nov 2023 at 22:22.
The following 3 users liked this post by Arthur Pape: