Originally Posted by
OldnGrounded
It would be a good idea to try to prepare, but it should be recognized that turning any random spaces -- including in existing medical facilities -- into effective isolation wards is far from a trivial task. And even if you have the physical plant, you still need trained personnel to care for the patients and for the facilities. If an effort like this is contemplated, the responsible parties should be in high gear already and be provided with plenty of resources.
Getting in front of the curve would seem prudent.
Cases ending in fatality take around 7 days on average to progress to conclusion from first symptoms. Symptoms are observed around 2 days after contracting the virus. Discounting the 2 day lag, then the available data from China in January is suggesting some things.
The case fatality rate stated at the end of January was that the CFR was lower that SARS, Great!. About 2 %, comparing total cases on 30th Jan to fatalities on the 30th January. So, what about the lag? Those that had succumbed by 30th January, contracted the virus around the 23rd January, and so the figures of cases on the earlier date are appropriate to use as the denominator when working out the CFR. ... Those that had died on 30th January, (213) came from a total case catchment on 23rd January (639). Now, before going off the deep end, this is telling us two things, the rate is probably higher than is being touted by WHO, CNN etc, considerably so. It also suggests that there was a lot of missing case data in the dataset, a lot or actual cases were possibly not being recorded at that time. How is that able to be deduced? shift the dates in question to the 4th February, and look back, as for the second chart below. That gives a CFR of 493/7700, or 6.4%, against 213/639, or 33.3%.
The take homes are:
- The figures are as good as the data capture and the subsequent analysis that is done;
- A 33% CFR would gain even the PRC Govt's attention, but would need to be reduced to avoid panic. Noting that twice as many people are normally admitted to critical care, that would have a high rate of all cases needing assistance. The analysis then would depend on the number of people that are getting symptoms to the extent they need hospital admission, which is a shorter lag than that for fatalities. The official figure is approximately 20% of todays cases are needing hospitalisation, but again, they contracted the virus 2 to 3 days before, and that is a bit more than half the current cases (4 Feb, 20,492 cases, 20% is.... 4098 cases. 2 Feb, 16884 cases, > 4098/16884= 24.3%). That is only about a 20% increase in the likely number of people needing ICU, so perhaps the 100K ICU beds total that exist in the US of A are more than adequate. For China, no wonder they are building new hospitals; they also need to build more funeral homes unfortunately. Every statistic is a family member, a tragedy and a loss to the community.
- Missing data is not all bad news, if more cases existed unreported, then the real CFR would be lower, although the spread would be higher. With a contagion that shows a capability to be easily spread, it would be comforting to know that the spread is much higher than reported, as yet there is no sign of real control of the progression in the hard hit communities.
- The international cases are still relatively low, and are not progressing quite like Wuhan has to date, but that may all change in the near future. Additional external person to person transmission has occurred in Thailand and in Singapore today, so that will add to the data and trends. Every day takes us closer to the point of global concern, where the fatalities start to occur to external populations that had no association with Wuhan directly. As of today, that has not happened, and it is not impossible that it will not happen, but that is unlikely, the most likely development is a start of fatalities later this week overseas, at which point the concern will be whether the rate is different to the PRC experience. There are various reasons why that may be the case, and that will be the point that the fire handles will be pulled out of self interest or not. To be effective, all the containment and protections need to be put in place before hand, to avoid saturation of the medical services. China may be able to put up a hospital in 10 days, but I doubt that many other places on the planet could do such a feat.
- The 3000 pax on the cruise ship in Japan probably would like to have made different choices in their travel plans. Many will not be positive, so far only 10 have been tested positive out of a fair testing %, but, they are all looking at free food and beer for the next couple of weeks from a single source. That is the level of disruption that we can look forward to without timely and reasonable protocols in place.
- When you board an RPT aircraft, whether your travel will be disrupted is dependent on everyone else in that tube being asymptomatic. The inconvenience is not as significant as the risk to self and to others from asymptomatic transfer and thereafter spread to those in your neck of the woods.
- By this Sunday, the data should indicate how bad this is going to be globally, we know it is tough in China to the local population in the current environment, with existing treatment. By then the international cases would be expected to show local fatalities. More data the better.
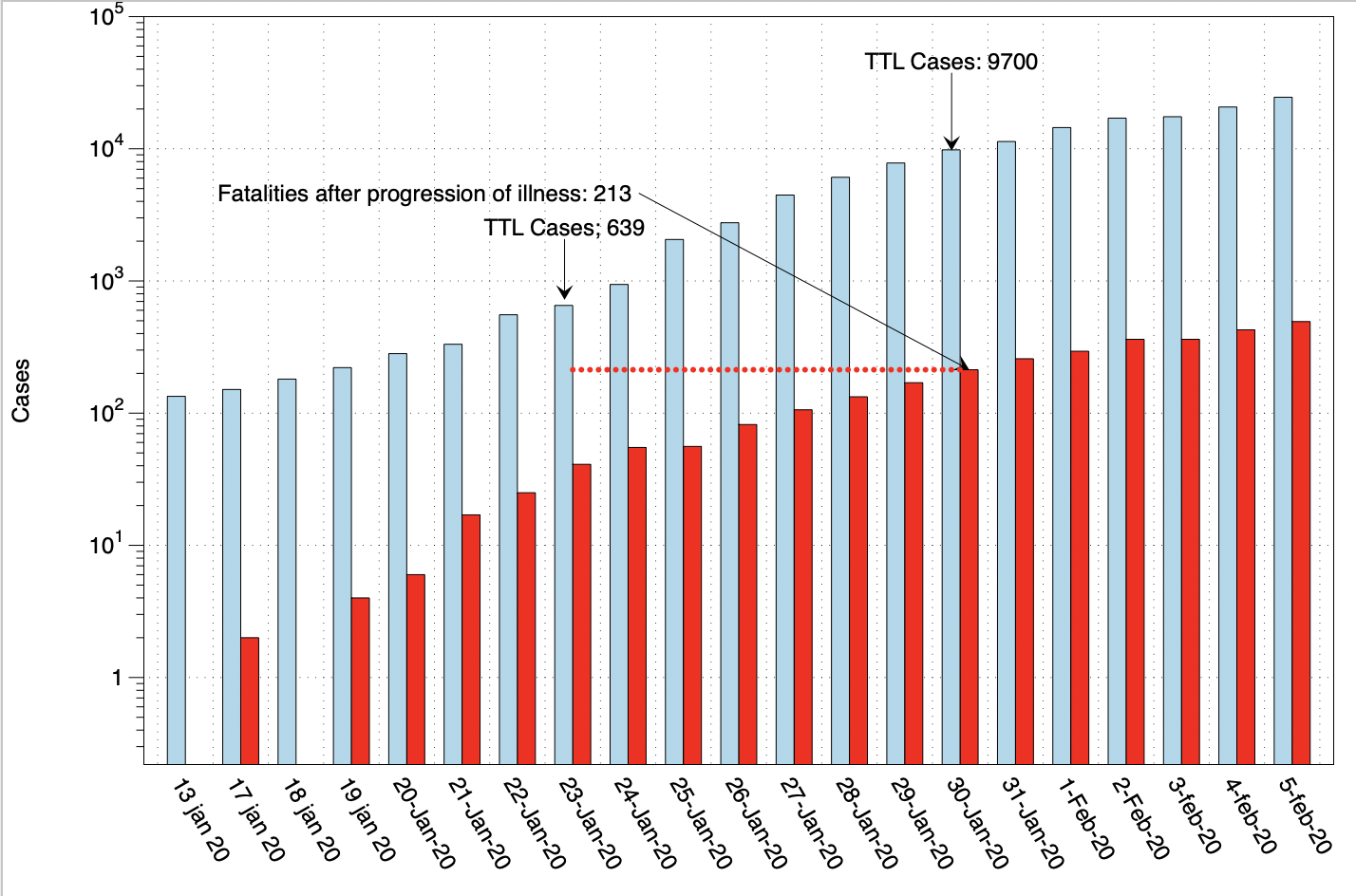

The prior charts are log scale for cases, to allow the data to be read, but they appear alarming as a result of that scale. To keep things in perspective, a normal scale of cases is below, of the same data.
The facts remain the same, it is quite possible that the case numbers out of China are well underreported, or alternatively the CFR is much higher than we want with a readily transmissible virus. Outside of China, transmissibility is entirely up to individuals as to how they behave and how they cope with infection control. Masks have some value, but the transmission from a contaminated surface (a "fomite") to the individual needs the action of the individual to complete as often as not. That is not saying gloves cure the problem, the problem is your own hand touching your face, to which end a mask of any sort at least is a reminder to "...be careful out there, it is a jungle..."
