


A109S Medevac Crash Brainerd Minnesota

Avoid imitations
Join Date: Nov 2000
Location: Wandering the FIR and cyberspace often at highly unsociable times
Posts: 14,573
Received 419 Likes
on
221 Posts
gulliBell, Let's hope so but when it comes to individual control inputs, I doubt a passenger would know the precise sequence of events.
There are far, far too many aircraft involved in "low vis" accidents of this nature.
There are far, far too many aircraft involved in "low vis" accidents of this nature.

"Just a pilot"
Perhaps as simple as autopilot failure, pilot misusing controls:
NTSB Identification: NYC06MA005
HISTORY OF FLIGHT
On October 7, 2005, at 2342 eastern daylight time, an Agusta 109E, N7YL, operated by CJ Systems Aviation Group Inc., was destroyed when it impacted trees and terrain in Smethport, Pennsylvania, while performing an instrument approach to Bradford Regional Airport (BFD), Bradford, Pennsylvania. The certificated commercial pilot was fatally injured. Night instrument meteorological conditions (IMC) prevailed, and an instrument flight rules (IFR) flight plan was filed for the flight that originated from Kane Community Hospital (PA91), Kane, Pennsylvania, at 2324. The positioning flight was conducted under 14 CFR Part 91.
In an interview, a mission flight nurse stated that he and another nurse were onboard the helicopter during a positioning flight from their base in Harborcreek, Pennsylvania, to Kane Community Hospital. Upon arrival at the hospital, he and the other nurse deplaned to prepare a patient for transport to Pittsburgh, Pennsylvania, while the helicopter departed for Bradford Airport to refuel.
Examination of radar and voice communication data provided by the Federal Aviation Administration (FAA) revealed that the helicopter departed Kane Hospital helipad and tracked the Copter GPS 246 Departure procedure course. The pilot contacted air traffic control (ATC), at 2324:47, stated that he had departed the hospital, and was "VFR to uh Bradford three thousand two hundred climbing to five."
Over the next 4 minutes, the pilot requested the instrument landing system (ILS) runway 32 approach to Bradford Regional Airport, and he and the controller discussed whether the helicopter would be vectored to the final approach course or if the full approach procedure would be flown.
The controller stated, "say your heading I've got you heading the wrong way for Bradford." The pilot replied that he was heading 246 degrees, which was prescribed in the procedure, but the controller questioned the response. The pilot reaffirmed his intention to fly to Bradford, and the controller assigned a 040-degree heading.
The pilot acknowledged the instructions; the helicopter then reversed direction, and assumed a northeasterly track. About 3 minutes later, the controller stated, "fly heading of zero eight five radar vectors runway three two I-L-S."
The pilot acknowledged the radio call, and the helicopter assumed an easterly track.
At 2339:01, the controller stated, "seven yankee lima fly heading of three four zero join the localizer report established please." At that time, the helicopter was at 5,000 feet, on an easterly track, about 1 mile west of the runway extended centerline, about 150 knots groundspeed. The pilot acknowledged the instructions.
The radar track depicted the helicopter on an easterly heading as it flew through the 322-degree final approach course, about 4 miles outside of the outer marker.
At 2340:03, the controller advised the pilot that the helicopter was "on the right side of the I-L-S," and the pilot acknowledged the call. At 2341:09, the controller asked if the pilot was established on the ILS. The pilot responded that he was "recapturing." The controller then asked if the pilot had said "affirmative," and the pilot replied "affirmative." At 0341:19, the controller transmitted, "Lifeguard seven yankee lima roger cleared I-L-S three two uh runway at Bradford uh maintain four thousand feet and uh report cancellation on this frequency..." The pilot read back the clearance at 0341:33. There were no further transmissions from the helicopter.
When the pilot replied "recapturing" the controller insisted the pilot respond "affirmative," which the pilot subsequently did.
At the time the controller advised that the helicopter was right of the localizer course, the radar track depicted the helicopter about midway through a left turn to about a 310-degree heading, at 5,000 feet, and about 1 mile east of the runway centerline.
The helicopter's track approached the localizer course centerline, and then turned sharply away from, and to the right of the inbound course. The radar target showed an approximate track of 100 degrees, when the target disappeared. During the 1 minute and 10 seconds following the pilot's acknowledgement of the 4,000-foot altitude assignment, the helicopter descended only 300 feet, slowed to approximately 65 knots groundspeed, and turned 140 degrees right of course.
The final three plots of the radar track showed a sharp left turn back towards the localizer course, and an approximate ground speed of 55 knots. The last radar plot was approximately over the crash site at 4,300 feet, about 1 mile east of the extended runway centerline, and 4 miles from the airport.
In an interview, a witness that lived approximately 1 mile from the crash site said that he did not see the helicopter, but heard it pass overhead. He said he was familiar with the sound, as he had lived close to the final approach course for runway 32 for many years.
The witness said the sound was louder than usual, and he felt the helicopter was closer to his home and lower than usual. The witness described the sound as smooth and continuous, with no change in aircraft noise. After the helicopter over flew his position, he heard the sound of an explosion.
On October 8, 2005, the FAA generated an alert notice at 0101, and a ground search for the helicopter began in the early morning hours of October 8, 2005. A search by air was not conducted due to weather. The helicopter wreckage was found on October 9, 2005, and was examined at the site on October 10, 2005.
The accident occurred during the hours of darkness approximately 40 degrees, 53 minutes north latitude, and 78 degrees, 06 minutes west longitude.
PERSONNEL INFORMATION
The pilot held a commercial pilot certificate with ratings for rotorcraft helicopter and instrument helicopter. The commercial certificate was issued February 10, 1979, and the instrument rating was added June 18, 1997. His most recent FAA second-class medical certificate was issued on October 19, 2004, and he reported 9,616 total hours of flight experience on that date.
The pilot's logbook was not recovered; however, some flight times were extracted from company records. In the 90 days prior to the accident, the pilot logged 56 hours, all of which was in the Augusta 109E. In this time period, he logged 25 hours of flight experience at night, 3 hours of simulated instrument experience, and 3 hours of actual instrument flight experience.
The company reported that the pilot had 110 total hours of instrument flight experience, and estimated that of this 70 hours were simulated instrument flight experience, and 40 hours were actual instrument flight experience. Later, the company reported that the pilot had accrued 100 hours of instrument flying experience, 10 hours of which was simulated.
AIRCRAFT INFORMATION
The helicopter was manufactured in 2001, and had accrued 1,905 total airframe hours. It was maintained under an Approved Aircraft Inspection Program (AAIP), and its most recent inspection was completed August 5, 2005.
The helicopter was equipped with an Integrated Flight Control System (IFCS). The system provided attitude automatic stabilization and automatic path control. Both stabilization and automatic path computation were actuated through the helipilot (autopilot) system and the flight director system.
A review of maintenance records revealed numerous entries related to autopilot malfunctions and failures. The malfunctions included erratic command bars on pilot and copilot displays, and uncommanded pitch and roll oscillations that occurred during preflight checks and also in flight. Over a 2-year span, 10 autopilot computers were changed on the accident helicopter due to their exposure to "high vibration levels."
A service bulletin (109EP-51) was released February 9, 2005, to address the vibration issues with the installation of shock-isolating mounts on the mounting trays for the autopilot computers. According to the site mechanic where the helicopter was based, he didn't recall having to change any computers once the service bulletin was applied.
METEOROLOGICAL INFORMATION
At 2337, the weather reported at Bradford Regional Airport included an overcast ceiling at 600 feet, with 2 1/2 miles of visibility in mist. The temperature was 50 degrees Fahrenheit, and the dew point was 48 degrees Fahrenheit.
WRECKAGE AND IMPACT INFORMATION
The helicopter impacted heavily wooded terrain about 2,000 feet elevation and all major components were accounted for at the scene. The initial impact point was in a treetop about 50 feet above the ground on level terrain. The wreckage path was about 180 feet long, and oriented about 100 degrees. The helicopter was fragmented, burned, and melted along the entire path. There were several pieces of angularly cut wood along the wreckage path, and several trees with fire damage and long angular slices along their trunks.
The wreckage path was documented at 1-foot increments called wreckage points (WP). At WP 33, a large tree, about 15 inches in diameter, was broken off about 25 feet above the ground. Sheets of composite material were embedded vertically into the trunk fracture.
The vertical fin was at WP 41. The tailboom was abeam the vertical fin, about 30 feet right of the wreckage path centerline. Structure that contained the number 1 hangar bearing was also at WP 41, 25 feet left of centerline. Both the left and the right antenna from the accident helicopter were destroyed by impact and postcrash fire.
The main wreckage, which consisted mostly of the main transmission with the mast and rotor head attached, was entangled at the base of three trees at WP 66. The cockpit and cabin area were consumed by fire, and all the flight and system instruments had been destroyed.
Because of impact and fire damage, control continuity could not be established. All flight controls, tubes, and bellcranks that were examined displayed impact damage and failures consistent with overload.
All four rotor blades were located at the site. They were extensively damaged by impact and fire. The red, white, and yellow blade grips were still attached to the rotor head. The blue blade grip, with damper attached, was located about 12 feet to the right of the transmission and rotor head.
All four main rotor blade spars were exposed, with the associated composite and honeycomb material scattered along the wreckage path.
Examination of the rotor head revealed that the red and white pitch change links were still attached to their hubs and the swashplate. The pitch change link for the yellow blade was broken at the swashplate, and the blue pitch change link was broken at the blade grip. All fractures were consistent with overload.
The red, white, and yellow dampers were still attached to the rotor head, but separated from their respective blade grips. The blue main rotor blade damper was separated from the rotor head, but still attached to its blade grip.
The engines were entangled in aircraft structure at WP 75, and both were extensively damaged by fire. The number one engine was largely intact. The number two engine was broken open, with internal components scattered on the ground.
Continuity of the powertrain could not be established. The combining gearbox was fractured into several pieces, and the oil cooler impeller was exposed. All drive couplings and driveshafts showed fracture surfaces that were consistent with impact and torsional overload.
A section of tree trunk, about 6 feet long and consistent with the fractured tree at WP 33, was found 180 feet beyond the initial point of impact. The trunk section was about 15 inches in diameter. The bark and wood along one side was shaved clean and displayed angular slices. There was aircraft structural sheet metal and associated hardware embedded in the wood.
TESTS AND RESEARCH
The engines were reexamined at Turbomeca, USA, Grand Prairie, Texas, on January 19, 2006, under the supervision of the FAA.
Examination of the number one engine revealed rotational tearing of the coupling at the accessory drive gearbox. The single-stage high-pressure turbine showed signs of rub on nozzle segments at the 1:00 o'clock position. The power turbine shaft had a torsional tear consistent with rotation and impact.
Examination of the number two engine revealed that the inlet axial compressor blades displayed impact damage and rotational tearing. The power turbine shaft was sheared and worn smooth from rotation at the accessory drive gearbox and the gas generator connection.
COMMUNICATION
A Safety Board air traffic control specialist convened an air traffic control group at Cleveland Air Route Traffic Control Center (ZOB), Oberlin, Ohio, on October 18, 2005. The group reviewed radar and voice communication recordings, collected documentation, conducted interviews, and the Safety Board specialist completed a factual report.
When questioned about the ILS runway 32 approach, the controller was unable to estimate the glideslope altitude at the point that the helicopter crossed the ILS localizer. Given an approach chart, he was able to identify the glideslope altitude at the outer marker as 3,333 feet. When he issued the approach clearance, the controller stated, "…cleared ILS three two uh runway at Bradford uh maintain four thousand feet." The controller was unable to explain what he intended by appending the 4,000 foot restriction to the approach clearance. He also stated that when he issued the approach clearance he had no feel for the relationship between the helicopter's altitude and the glideslope altitude at the helicopter's location.
According to FAAO 7110.65, the controller shall, "Assign headings that will permit final approach course interception on a track that does not exceed the interception angles specified in the TBL 5-9-1." The appropriate intercept angle values were 30 degrees for fixed-wing aircraft and 45 degrees for helicopters.
According to FAAO 7110.65, paragraph 5-9-1(b), controllers should position aircraft as follows: "For a precision approach, at an altitude not above the glideslope/glidepath or below the minimum glideslope intercept altitude specified on the approach procedure chart."
The FAA conducted a postaccident flight inspection of the ILS runway 32 approach at Bradford Regional Airport, and the results were "Satisfactory," with no deficiencies noted.
MEDICAL AND PATHOLOGICAL INFORMATION
The FAA Bioaeronautical Sciences Research Laboratory, Oklahoma City, Oklahoma, performed the toxicological testing of the pilot. Chlorpheniramine, an antihistamine, was detected in the heart and liver.
The antihistamine chlorpheniramine was available over-the-counter under the commercial name Chlor-trimeton. According to the manufacturer, the side effects associated with chlorpheniramine included headache, fatigue, and dizziness. Among the warnings listed for consumers was, "Use caution when driving a motor vehicle or operating machinery."
According to his supervisor, the pilot was very physically fit, but "had a sinus condition on occasion." The flight nurse also stated the pilot "always seemed to have sinus problems."
The Mount Nittany Medical Center, State College, Pennsylvania, performed an autopsy on the pilot.
ADDITIONAL INFORMATION
According to the operator's director of training, as well as pilots employed by the airframe manufacturer, after the helicopter flew through the final approach course, and turned to the west, the autopilot could still capture the localizer course. However, once the helicopter was in the vicinity of the localizer course, and above the glideslope, the autopilot would be unable to capture the glideslope.
If altitude hold remained engaged at that point of the flight, and the pilot reduced collective to capture the glideslope, the autopilot would adjust pitch in an effort to maintain the selected altitude.
The Flight Safety Foundation publication Helicopter Safety, May-June 1997, Helicopter Autopilots Demand Careful Management, discussed some scenarios of "autopilot mismanagement."
One scenario described was in a flight simulator, where the crew reached a selected altitude, but no corresponding collective/power adjustment was made. Therefore, "As the aircraft approached the target altitude, the altitude preselect feature enunciated a "capture." Illumination of the altitude-hold button on the flight director followed. A few seconds later, the gear-up warning horn began to sound, triggered by airspeed below [60 knots].
"Surprised, the pilots scanned the instruments and saw that the airspeed was rapidly decreasing, the aircraft pitch attitude was very nose-high and the aircraft was in a descent…Therefore, the autopilot attempted to maintain altitude by increasing pitch attitude, thus decreasing the airspeed. At the selected power setting, the descent could not be prevented by the autopilot and airspeed decreased until the gear-up warning horn alerted the pilots."
Another scenario took place on an actual flight. In this scenario "The [pilot] was surprised to see that the attitude directional indicator (ADI) was indicating extreme nose-up pitch. A quick scan of other instruments showed that the airspeed was rapidly decreasing, and the vertical speed indicator was showing a descent. The pilot quickly took manual control of the aircraft; increasing the collective pitch and lowering the aircraft nose to recover from the unusual attitude. He succeeded, but afterwards was shaken by the event."
On April 17, 2007, flight simulations were conducted in a Level D full-motion simulator at the Augusta-Westland Training Academy, Sesto, Italy, utilizing the radar data from the accident flight. While the instrument displays in the simulator differed from the accident helicopter, the stabilization and autopilot systems were identical.
Four simulations were conducted, initiated from the same point at 145 knots at 5,000 feet, but each with different selection times for the autopilot modes (Heading, Altitude, Approach). A fifth simulation was conducted at a lower speed of 110 knots and with Approach (ILS) mode selected prior to reaching the localizer course.
During the first simulation, approach mode was selected as the helicopter passed through the localizer centerline. The autopilot captured the localizer, but the turn resulted in a wide overshoot. Later in the approach, the autopilot captured the glideslope, but the helicopter pitched 10 degrees nose-down, descended at 3,000 feet per minute, and reached the simulator's maximum airspeed of 183 knots. The simulation was stopped 950 feet above ground level.
During the fifth simulation, the approach mode was selected prior to localizer intercept. The autopilot captured and tracked both the localizer and glide slope, and automatically disengaged the heading and altitude modes.
During simulations 2, 3, and 4, the turns to intercept the localizer course were completed in heading mode, and approach mode was selected after completion of the turn. The autopilot captured the localizer, but not the glideslope. All three approaches resulted in a "slight" reduction in altitude, pitch up attitude of 10 to 30 degrees, slowing to below 30 knots, and finally a vertical descent.
The flight profile and vertical fall of the last phase of simulations 2, 3, and 4 were consistent with the accident flight and ultimate position of the wreckage, and coincided closely with the last radar sweep. At the end of simulation 3, the pilot recovered the helicopter and resumed controlled flight.
NTSB Identification: NYC06MA005
HISTORY OF FLIGHT
On October 7, 2005, at 2342 eastern daylight time, an Agusta 109E, N7YL, operated by CJ Systems Aviation Group Inc., was destroyed when it impacted trees and terrain in Smethport, Pennsylvania, while performing an instrument approach to Bradford Regional Airport (BFD), Bradford, Pennsylvania. The certificated commercial pilot was fatally injured. Night instrument meteorological conditions (IMC) prevailed, and an instrument flight rules (IFR) flight plan was filed for the flight that originated from Kane Community Hospital (PA91), Kane, Pennsylvania, at 2324. The positioning flight was conducted under 14 CFR Part 91.
In an interview, a mission flight nurse stated that he and another nurse were onboard the helicopter during a positioning flight from their base in Harborcreek, Pennsylvania, to Kane Community Hospital. Upon arrival at the hospital, he and the other nurse deplaned to prepare a patient for transport to Pittsburgh, Pennsylvania, while the helicopter departed for Bradford Airport to refuel.
Examination of radar and voice communication data provided by the Federal Aviation Administration (FAA) revealed that the helicopter departed Kane Hospital helipad and tracked the Copter GPS 246 Departure procedure course. The pilot contacted air traffic control (ATC), at 2324:47, stated that he had departed the hospital, and was "VFR to uh Bradford three thousand two hundred climbing to five."
Over the next 4 minutes, the pilot requested the instrument landing system (ILS) runway 32 approach to Bradford Regional Airport, and he and the controller discussed whether the helicopter would be vectored to the final approach course or if the full approach procedure would be flown.
The controller stated, "say your heading I've got you heading the wrong way for Bradford." The pilot replied that he was heading 246 degrees, which was prescribed in the procedure, but the controller questioned the response. The pilot reaffirmed his intention to fly to Bradford, and the controller assigned a 040-degree heading.
The pilot acknowledged the instructions; the helicopter then reversed direction, and assumed a northeasterly track. About 3 minutes later, the controller stated, "fly heading of zero eight five radar vectors runway three two I-L-S."
The pilot acknowledged the radio call, and the helicopter assumed an easterly track.
At 2339:01, the controller stated, "seven yankee lima fly heading of three four zero join the localizer report established please." At that time, the helicopter was at 5,000 feet, on an easterly track, about 1 mile west of the runway extended centerline, about 150 knots groundspeed. The pilot acknowledged the instructions.
The radar track depicted the helicopter on an easterly heading as it flew through the 322-degree final approach course, about 4 miles outside of the outer marker.
At 2340:03, the controller advised the pilot that the helicopter was "on the right side of the I-L-S," and the pilot acknowledged the call. At 2341:09, the controller asked if the pilot was established on the ILS. The pilot responded that he was "recapturing." The controller then asked if the pilot had said "affirmative," and the pilot replied "affirmative." At 0341:19, the controller transmitted, "Lifeguard seven yankee lima roger cleared I-L-S three two uh runway at Bradford uh maintain four thousand feet and uh report cancellation on this frequency..." The pilot read back the clearance at 0341:33. There were no further transmissions from the helicopter.
When the pilot replied "recapturing" the controller insisted the pilot respond "affirmative," which the pilot subsequently did.
At the time the controller advised that the helicopter was right of the localizer course, the radar track depicted the helicopter about midway through a left turn to about a 310-degree heading, at 5,000 feet, and about 1 mile east of the runway centerline.
The helicopter's track approached the localizer course centerline, and then turned sharply away from, and to the right of the inbound course. The radar target showed an approximate track of 100 degrees, when the target disappeared. During the 1 minute and 10 seconds following the pilot's acknowledgement of the 4,000-foot altitude assignment, the helicopter descended only 300 feet, slowed to approximately 65 knots groundspeed, and turned 140 degrees right of course.
The final three plots of the radar track showed a sharp left turn back towards the localizer course, and an approximate ground speed of 55 knots. The last radar plot was approximately over the crash site at 4,300 feet, about 1 mile east of the extended runway centerline, and 4 miles from the airport.
In an interview, a witness that lived approximately 1 mile from the crash site said that he did not see the helicopter, but heard it pass overhead. He said he was familiar with the sound, as he had lived close to the final approach course for runway 32 for many years.
The witness said the sound was louder than usual, and he felt the helicopter was closer to his home and lower than usual. The witness described the sound as smooth and continuous, with no change in aircraft noise. After the helicopter over flew his position, he heard the sound of an explosion.
On October 8, 2005, the FAA generated an alert notice at 0101, and a ground search for the helicopter began in the early morning hours of October 8, 2005. A search by air was not conducted due to weather. The helicopter wreckage was found on October 9, 2005, and was examined at the site on October 10, 2005.
The accident occurred during the hours of darkness approximately 40 degrees, 53 minutes north latitude, and 78 degrees, 06 minutes west longitude.
PERSONNEL INFORMATION
The pilot held a commercial pilot certificate with ratings for rotorcraft helicopter and instrument helicopter. The commercial certificate was issued February 10, 1979, and the instrument rating was added June 18, 1997. His most recent FAA second-class medical certificate was issued on October 19, 2004, and he reported 9,616 total hours of flight experience on that date.
The pilot's logbook was not recovered; however, some flight times were extracted from company records. In the 90 days prior to the accident, the pilot logged 56 hours, all of which was in the Augusta 109E. In this time period, he logged 25 hours of flight experience at night, 3 hours of simulated instrument experience, and 3 hours of actual instrument flight experience.
The company reported that the pilot had 110 total hours of instrument flight experience, and estimated that of this 70 hours were simulated instrument flight experience, and 40 hours were actual instrument flight experience. Later, the company reported that the pilot had accrued 100 hours of instrument flying experience, 10 hours of which was simulated.
AIRCRAFT INFORMATION
The helicopter was manufactured in 2001, and had accrued 1,905 total airframe hours. It was maintained under an Approved Aircraft Inspection Program (AAIP), and its most recent inspection was completed August 5, 2005.
The helicopter was equipped with an Integrated Flight Control System (IFCS). The system provided attitude automatic stabilization and automatic path control. Both stabilization and automatic path computation were actuated through the helipilot (autopilot) system and the flight director system.
A review of maintenance records revealed numerous entries related to autopilot malfunctions and failures. The malfunctions included erratic command bars on pilot and copilot displays, and uncommanded pitch and roll oscillations that occurred during preflight checks and also in flight. Over a 2-year span, 10 autopilot computers were changed on the accident helicopter due to their exposure to "high vibration levels."
A service bulletin (109EP-51) was released February 9, 2005, to address the vibration issues with the installation of shock-isolating mounts on the mounting trays for the autopilot computers. According to the site mechanic where the helicopter was based, he didn't recall having to change any computers once the service bulletin was applied.
METEOROLOGICAL INFORMATION
At 2337, the weather reported at Bradford Regional Airport included an overcast ceiling at 600 feet, with 2 1/2 miles of visibility in mist. The temperature was 50 degrees Fahrenheit, and the dew point was 48 degrees Fahrenheit.
WRECKAGE AND IMPACT INFORMATION
The helicopter impacted heavily wooded terrain about 2,000 feet elevation and all major components were accounted for at the scene. The initial impact point was in a treetop about 50 feet above the ground on level terrain. The wreckage path was about 180 feet long, and oriented about 100 degrees. The helicopter was fragmented, burned, and melted along the entire path. There were several pieces of angularly cut wood along the wreckage path, and several trees with fire damage and long angular slices along their trunks.
The wreckage path was documented at 1-foot increments called wreckage points (WP). At WP 33, a large tree, about 15 inches in diameter, was broken off about 25 feet above the ground. Sheets of composite material were embedded vertically into the trunk fracture.
The vertical fin was at WP 41. The tailboom was abeam the vertical fin, about 30 feet right of the wreckage path centerline. Structure that contained the number 1 hangar bearing was also at WP 41, 25 feet left of centerline. Both the left and the right antenna from the accident helicopter were destroyed by impact and postcrash fire.
The main wreckage, which consisted mostly of the main transmission with the mast and rotor head attached, was entangled at the base of three trees at WP 66. The cockpit and cabin area were consumed by fire, and all the flight and system instruments had been destroyed.
Because of impact and fire damage, control continuity could not be established. All flight controls, tubes, and bellcranks that were examined displayed impact damage and failures consistent with overload.
All four rotor blades were located at the site. They were extensively damaged by impact and fire. The red, white, and yellow blade grips were still attached to the rotor head. The blue blade grip, with damper attached, was located about 12 feet to the right of the transmission and rotor head.
All four main rotor blade spars were exposed, with the associated composite and honeycomb material scattered along the wreckage path.
Examination of the rotor head revealed that the red and white pitch change links were still attached to their hubs and the swashplate. The pitch change link for the yellow blade was broken at the swashplate, and the blue pitch change link was broken at the blade grip. All fractures were consistent with overload.
The red, white, and yellow dampers were still attached to the rotor head, but separated from their respective blade grips. The blue main rotor blade damper was separated from the rotor head, but still attached to its blade grip.
The engines were entangled in aircraft structure at WP 75, and both were extensively damaged by fire. The number one engine was largely intact. The number two engine was broken open, with internal components scattered on the ground.
Continuity of the powertrain could not be established. The combining gearbox was fractured into several pieces, and the oil cooler impeller was exposed. All drive couplings and driveshafts showed fracture surfaces that were consistent with impact and torsional overload.
A section of tree trunk, about 6 feet long and consistent with the fractured tree at WP 33, was found 180 feet beyond the initial point of impact. The trunk section was about 15 inches in diameter. The bark and wood along one side was shaved clean and displayed angular slices. There was aircraft structural sheet metal and associated hardware embedded in the wood.
TESTS AND RESEARCH
The engines were reexamined at Turbomeca, USA, Grand Prairie, Texas, on January 19, 2006, under the supervision of the FAA.
Examination of the number one engine revealed rotational tearing of the coupling at the accessory drive gearbox. The single-stage high-pressure turbine showed signs of rub on nozzle segments at the 1:00 o'clock position. The power turbine shaft had a torsional tear consistent with rotation and impact.
Examination of the number two engine revealed that the inlet axial compressor blades displayed impact damage and rotational tearing. The power turbine shaft was sheared and worn smooth from rotation at the accessory drive gearbox and the gas generator connection.
COMMUNICATION
A Safety Board air traffic control specialist convened an air traffic control group at Cleveland Air Route Traffic Control Center (ZOB), Oberlin, Ohio, on October 18, 2005. The group reviewed radar and voice communication recordings, collected documentation, conducted interviews, and the Safety Board specialist completed a factual report.
When questioned about the ILS runway 32 approach, the controller was unable to estimate the glideslope altitude at the point that the helicopter crossed the ILS localizer. Given an approach chart, he was able to identify the glideslope altitude at the outer marker as 3,333 feet. When he issued the approach clearance, the controller stated, "…cleared ILS three two uh runway at Bradford uh maintain four thousand feet." The controller was unable to explain what he intended by appending the 4,000 foot restriction to the approach clearance. He also stated that when he issued the approach clearance he had no feel for the relationship between the helicopter's altitude and the glideslope altitude at the helicopter's location.
According to FAAO 7110.65, the controller shall, "Assign headings that will permit final approach course interception on a track that does not exceed the interception angles specified in the TBL 5-9-1." The appropriate intercept angle values were 30 degrees for fixed-wing aircraft and 45 degrees for helicopters.
According to FAAO 7110.65, paragraph 5-9-1(b), controllers should position aircraft as follows: "For a precision approach, at an altitude not above the glideslope/glidepath or below the minimum glideslope intercept altitude specified on the approach procedure chart."
The FAA conducted a postaccident flight inspection of the ILS runway 32 approach at Bradford Regional Airport, and the results were "Satisfactory," with no deficiencies noted.
MEDICAL AND PATHOLOGICAL INFORMATION
The FAA Bioaeronautical Sciences Research Laboratory, Oklahoma City, Oklahoma, performed the toxicological testing of the pilot. Chlorpheniramine, an antihistamine, was detected in the heart and liver.
The antihistamine chlorpheniramine was available over-the-counter under the commercial name Chlor-trimeton. According to the manufacturer, the side effects associated with chlorpheniramine included headache, fatigue, and dizziness. Among the warnings listed for consumers was, "Use caution when driving a motor vehicle or operating machinery."
According to his supervisor, the pilot was very physically fit, but "had a sinus condition on occasion." The flight nurse also stated the pilot "always seemed to have sinus problems."
The Mount Nittany Medical Center, State College, Pennsylvania, performed an autopsy on the pilot.
ADDITIONAL INFORMATION
According to the operator's director of training, as well as pilots employed by the airframe manufacturer, after the helicopter flew through the final approach course, and turned to the west, the autopilot could still capture the localizer course. However, once the helicopter was in the vicinity of the localizer course, and above the glideslope, the autopilot would be unable to capture the glideslope.
If altitude hold remained engaged at that point of the flight, and the pilot reduced collective to capture the glideslope, the autopilot would adjust pitch in an effort to maintain the selected altitude.
The Flight Safety Foundation publication Helicopter Safety, May-June 1997, Helicopter Autopilots Demand Careful Management, discussed some scenarios of "autopilot mismanagement."
One scenario described was in a flight simulator, where the crew reached a selected altitude, but no corresponding collective/power adjustment was made. Therefore, "As the aircraft approached the target altitude, the altitude preselect feature enunciated a "capture." Illumination of the altitude-hold button on the flight director followed. A few seconds later, the gear-up warning horn began to sound, triggered by airspeed below [60 knots].
"Surprised, the pilots scanned the instruments and saw that the airspeed was rapidly decreasing, the aircraft pitch attitude was very nose-high and the aircraft was in a descent…Therefore, the autopilot attempted to maintain altitude by increasing pitch attitude, thus decreasing the airspeed. At the selected power setting, the descent could not be prevented by the autopilot and airspeed decreased until the gear-up warning horn alerted the pilots."
Another scenario took place on an actual flight. In this scenario "The [pilot] was surprised to see that the attitude directional indicator (ADI) was indicating extreme nose-up pitch. A quick scan of other instruments showed that the airspeed was rapidly decreasing, and the vertical speed indicator was showing a descent. The pilot quickly took manual control of the aircraft; increasing the collective pitch and lowering the aircraft nose to recover from the unusual attitude. He succeeded, but afterwards was shaken by the event."
On April 17, 2007, flight simulations were conducted in a Level D full-motion simulator at the Augusta-Westland Training Academy, Sesto, Italy, utilizing the radar data from the accident flight. While the instrument displays in the simulator differed from the accident helicopter, the stabilization and autopilot systems were identical.
Four simulations were conducted, initiated from the same point at 145 knots at 5,000 feet, but each with different selection times for the autopilot modes (Heading, Altitude, Approach). A fifth simulation was conducted at a lower speed of 110 knots and with Approach (ILS) mode selected prior to reaching the localizer course.
During the first simulation, approach mode was selected as the helicopter passed through the localizer centerline. The autopilot captured the localizer, but the turn resulted in a wide overshoot. Later in the approach, the autopilot captured the glideslope, but the helicopter pitched 10 degrees nose-down, descended at 3,000 feet per minute, and reached the simulator's maximum airspeed of 183 knots. The simulation was stopped 950 feet above ground level.
During the fifth simulation, the approach mode was selected prior to localizer intercept. The autopilot captured and tracked both the localizer and glide slope, and automatically disengaged the heading and altitude modes.
During simulations 2, 3, and 4, the turns to intercept the localizer course were completed in heading mode, and approach mode was selected after completion of the turn. The autopilot captured the localizer, but not the glideslope. All three approaches resulted in a "slight" reduction in altitude, pitch up attitude of 10 to 30 degrees, slowing to below 30 knots, and finally a vertical descent.
The flight profile and vertical fall of the last phase of simulations 2, 3, and 4 were consistent with the accident flight and ultimate position of the wreckage, and coincided closely with the last radar sweep. At the end of simulation 3, the pilot recovered the helicopter and resumed controlled flight.
Single Pilot IFR in a helicopter at night in bad weather is a tough chore.
Anything that goes wrong....no matter how slight....tremendously increases the difficulty.
Be it caused by the Aircraft, its systems, external causes, or self induced....it can lead to real problems.
Question: Why not route east out of Kane and get radar vectors to a straight in for the ILS 32 approach at Bradford?
We are not talking about a very long distance between the two places.
That would have made the process much simpler and provide a bit of time to get it all sorted out.
Knowing the crossing height at the LOM or OM combined with DME data and other information would have facilitated a better approach.
The GPS could be used to assist in Situational Awareness as well.
https://flightaware.com/resources/ai...LOC+RWY+32/pdf
Anything that goes wrong....no matter how slight....tremendously increases the difficulty.
Be it caused by the Aircraft, its systems, external causes, or self induced....it can lead to real problems.
Question: Why not route east out of Kane and get radar vectors to a straight in for the ILS 32 approach at Bradford?
We are not talking about a very long distance between the two places.
That would have made the process much simpler and provide a bit of time to get it all sorted out.
Knowing the crossing height at the LOM or OM combined with DME data and other information would have facilitated a better approach.
The GPS could be used to assist in Situational Awareness as well.
https://flightaware.com/resources/ai...LOC+RWY+32/pdf
Last edited by SASless; 1st Jul 2019 at 14:42.
Devil49 - that crash report highlights exactly what I was trying to explain to Sasless - a 3-axis AP needs very good awareness and knowledge of how the system works if it is to be safely used in a high pressure SP IFR situation. It is too easy to presume that the 'automatic' capture for LOC and GS will work without intervention or monitoring.
Crab,
No explaining needed for me to understand....as I flew two types of aircraft with a three axis auto-pilot and if you remember my posts.
Also...recall I did not disagree with what you had to say....but did say it requires a pilot to fully understand how his particular aircraft responds to control inputs....either human or by avionic system.
That takes education, training, and practice.
As a Sim Instructor on the 212/412 and 76....I have observed many (far too many actually) well experienced working Pilots, single and two pilot crewing, fail to raise the Collective when performing a Missed Approach.
The usual warning clue was when there was no briefing or the Missed Approach part of the brief was omitted.
In my Sim....that guaranteed there would be a need to perform the Missed because I would disappear the airfield completely.
Sometimes in real life even....you have to declare a missed approach and go around....it helps to be prepared.
I somehow wonder if this might have been the cause of this latest 109 crash.
The symptoms are at DH (and if you are sneaking a bit) well below DH, the pilot decides to go around....either hits the GA Button and the aircraft pitches up, and without a proper Collective/Power addition or manually adjusts the pitch attitude and does not add power or enough power....the aircraft slows, the autopilot loses ability to control the machine and the Pilot is confronted with an unusual attitude, low and decreasing airspeed, and low power setting....and in this case in the dark and in cloud/fog perhaps. Usually it has a very bad outcome.
I taught an assertive response for a missed approach....as once taught back in the dark ages where we hand flew machines with basic instruments.....that being adding power first and to a predetermined power setting....adjusting the pitch attitude to a predetermined position and establishing Vbroc and climb rate. I also advocated flying the machine to 500 feet AGL before getting involved in collateral tasks.
No explaining needed for me to understand....as I flew two types of aircraft with a three axis auto-pilot and if you remember my posts.
Also...recall I did not disagree with what you had to say....but did say it requires a pilot to fully understand how his particular aircraft responds to control inputs....either human or by avionic system.
That takes education, training, and practice.
As a Sim Instructor on the 212/412 and 76....I have observed many (far too many actually) well experienced working Pilots, single and two pilot crewing, fail to raise the Collective when performing a Missed Approach.
The usual warning clue was when there was no briefing or the Missed Approach part of the brief was omitted.
In my Sim....that guaranteed there would be a need to perform the Missed because I would disappear the airfield completely.
Sometimes in real life even....you have to declare a missed approach and go around....it helps to be prepared.
I somehow wonder if this might have been the cause of this latest 109 crash.
The symptoms are at DH (and if you are sneaking a bit) well below DH, the pilot decides to go around....either hits the GA Button and the aircraft pitches up, and without a proper Collective/Power addition or manually adjusts the pitch attitude and does not add power or enough power....the aircraft slows, the autopilot loses ability to control the machine and the Pilot is confronted with an unusual attitude, low and decreasing airspeed, and low power setting....and in this case in the dark and in cloud/fog perhaps. Usually it has a very bad outcome.
I taught an assertive response for a missed approach....as once taught back in the dark ages where we hand flew machines with basic instruments.....that being adding power first and to a predetermined power setting....adjusting the pitch attitude to a predetermined position and establishing Vbroc and climb rate. I also advocated flying the machine to 500 feet AGL before getting involved in collateral tasks.
I agree SAS - it's down to education, training and practice but since civil type rating is a very quick process compared to converting to a new type in the military and there often aren't the non-revenue hours to give the practice, is it any wonder that pilots don't really know their AP systems?
Having taught on the 365N3 (3-axis) and as a recent convert to the 412 (again 3-axis) I am very comfortable with using the AP but that is after 500 hours of instructing it on the N3.
Although helping the cyclic channel capture the GS by lowering the lever and assisting the go-around by raising it are what would be considered 'normal' helicopter control inputs (ie what tyou would do if you were flying it manually), it is the conflicting element of controlling IAS with collective on approach that I believe causes problems.
It is the 'half' level of automation that is dangerous - it lulls you into a false sense of security because the AP is doing the hard work for you (where you would otherwise be working quite hard, especially in difficult conditions) and there is the problem of under-arousal at a critical stage of flight ie not visual at DA/DH.
Add in fatigue and body clock issues and its just a question of when not if.
Having taught on the 365N3 (3-axis) and as a recent convert to the 412 (again 3-axis) I am very comfortable with using the AP but that is after 500 hours of instructing it on the N3.
Although helping the cyclic channel capture the GS by lowering the lever and assisting the go-around by raising it are what would be considered 'normal' helicopter control inputs (ie what tyou would do if you were flying it manually), it is the conflicting element of controlling IAS with collective on approach that I believe causes problems.
It is the 'half' level of automation that is dangerous - it lulls you into a false sense of security because the AP is doing the hard work for you (where you would otherwise be working quite hard, especially in difficult conditions) and there is the problem of under-arousal at a critical stage of flight ie not visual at DA/DH.
Add in fatigue and body clock issues and its just a question of when not if.
Avoid imitations
Join Date: Nov 2000
Location: Wandering the FIR and cyberspace often at highly unsociable times
Posts: 14,573
Received 419 Likes
on
221 Posts
Crab, I concur.
As I always say, VFR helicopter flying is relatively straightforward. IFR helicopter flying slightly less so. Changing from VFR to IFR or from IFR to VFR is the tricky bit and it still tends to catch some pilots out.
As I always say, VFR helicopter flying is relatively straightforward. IFR helicopter flying slightly less so. Changing from VFR to IFR or from IFR to VFR is the tricky bit and it still tends to catch some pilots out.
Sometimes in real life even....you have to declare a missed approach and go around....it helps to be prepared.
Worse than flying a 3-axis AP, where ideally you should be familiar with its logic, is flying a 4-axis AP in 3-axis and jumping between the two. CHC showed us that in Sumburgh 6 years ago.
A109E Takeoff Go Around Limitation
I received a SPIFR qualifications in the B-230UT, A-109E and the EC-135P2/T2. All aircraft were equipped with 3 axis autopilots. Coupled ILS approaches were straight forward. As the glide slope was captured collective/power was set to achieve the desired approach speed. The specific autopilot installed by A109E (Duke Lifeflight) autopilot was an adaptation of a fixed wing unit. The A109E autopilot had a placarded limitation on the use of the take off/go around mode. Specifically, a placard limited the use to airspeeds greater than 120 KIAS. Attempted use at 70KIAS resulted in some very extreme attitude excursions. Has anyone one else experienced this?
I received a SPIFR qualifications in the B-230UT, A-109E and the EC-135P2/T2. All aircraft were equipped with 3 axis autopilots. Coupled ILS approaches were straight forward. As the glide slope was captured collective/power was set to achieve the desired approach speed. The specific autopilot installed by A109E (Duke Lifeflight) autopilot was an adaptation of a fixed wing unit. The A109E autopilot had a placarded limitation on the use of the take off/go around mode. Specifically, a placard limited the use to airspeeds greater than 120 KIAS. Attempted use at 70KIAS resulted in some very extreme attitude excursions. Has anyone one else experienced this?
There are two different wiring versions and they do different things when GA is pushed. Only the later version has the above note. Not sure about the 109S but the E and S are nearly identical electrically.
My experience teaching in the simulator is very similar to SASless. Trainees just don't understand the flight director and autopilot systems sufficiently well to be competent at using it. A lot of trainees need to be talked through the instrument approach by the instructor, step-by-step. "Now push this button", "now watch for the...", "now is a good time to do the before landing checks" etc etc. If you don't tell them what to do and when, they simply get overwhelmed. Another common error is flying level at 200' DH waiting to get visual. They slow down. And slow down some more. The nose pitches up slowly at first, and then all of a sudden, big nose pitch up and crash. And these are not initial issue IR applicants, they are annual recurrent, command qualified. The average competency is very low.
IMHO, the EMS SPIFR community is an accident waiting to happen. It�s hard to believe, in such a high workload environment with very little room for error, operators and the FAA do not demand overwhelming procedural standardization. Airlines have operated this way for years.
For example, an approach checklist from an EMS operator is approach-type generic, completely ignores use of automation, and lacks any specificity to actual installed avionics.
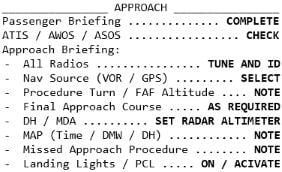
For example, an approach checklist from an EMS operator is approach-type generic, completely ignores use of automation, and lacks any specificity to actual installed avionics.
Last edited by JimEli; 3rd Jul 2019 at 12:58. Reason: added example checklist
Join Date: Feb 2001
Location: Europe
Posts: 535
Likes: 0
Received 0 Likes
on
0 Posts
Surely the fact that one needs to pull substantial power to go around at the bottom of an aborted ILS should be pretty obvious? Quite frankly if it�s not, a pilot should lose his IR until convincingly retrained. A 3 axis autopilot as on a 109 is not exactly basic hand flying on raw data.
I suggest IR proficiency checks should include the ability to uncouple and hand fly away if not visual at the bottom of an ILS. At least that would reinforce understanding of the basics. Surely many must agree?
I suggest IR proficiency checks should include the ability to uncouple and hand fly away if not visual at the bottom of an ILS. At least that would reinforce understanding of the basics. Surely many must agree?
Yes. A manually flown approach must also be demonstrated. Sometimes a manually flown approach is more successful than a coupled approach because there is less reliance on knowing what FD buttons to push, and when. Especially with a single engine missed approach, some trainees don't realize that the AP doesn't know whether one or two engines are working, leading to some interesting outcomes when the GA button is pushed.
I work on fixed wing air ambulance in the UK and look in sadness and horror at the number of crashes or major incidients in the rotary wing EMS community particulary in the US. Reading both professional journals and other sources, the number of people killed over recent years in these incidents I'm afraid and I maybe flamed here that sometimes that some companies financial imperative may outweigh good judgemnt and lead to inadvertant pressuring the flightcrews to make decisions that on other days in other places that they would not make. There is debate in the USA in some states at the moment about costs to patients for such flights either borne by the patients or their insurers.
https://abcnews.go.com/Health/doctor...ry?id=58125900
https://www.latimes.com/business/la-...611-story.html
The statistics from what I can find are between 2010 to 16 there were 46 accidents/incidents in which 20 had fatalities involved and in that a total of 50 crew and patients died.
https://abcnews.go.com/Health/doctor...ry?id=58125900
https://www.latimes.com/business/la-...611-story.html
The statistics from what I can find are between 2010 to 16 there were 46 accidents/incidents in which 20 had fatalities involved and in that a total of 50 crew and patients died.