


Flights from China

Join Date: Sep 2017
Location: Europe
Posts: 1,674
Likes: 0
Received 0 Likes
on
0 Posts
One bright spot is the Chinese habit of wearing a mask when ill to prevent the unchecked cloud of virus in every exhalation. That particular habit is something that the government would be wise to promote on TV etc.
Perhaps nature is telling us a little more loudly.
In times past serious viruses were fought with isolation and eventually defeated.
Perhaps better hygiene at a personal level, which is horrible in certain countries, will when combined with travel restrictions help out this time.

In epidemiology super-spreaders are not a hypothesis; they are known and documented phenomenon dating back to 'Typhoid Mary'. Super spreader events have been documented in both major previous coronavirus outbreaks - SARS and MERS.
Have a read of Stein's 2010 'Super-spreaders in infectious diseases' or Chun's 2016 'Understanding and Modeling the Super-spreading Events of the Middle East Respiratory Syndrome Outbreak in Korea' if you want to inform yourself.
If you want to argue the toss take it up with your local School of Epidemiology.
Have a read of Stein's 2010 'Super-spreaders in infectious diseases' or Chun's 2016 'Understanding and Modeling the Super-spreading Events of the Middle East Respiratory Syndrome Outbreak in Korea' if you want to inform yourself.
If you want to argue the toss take it up with your local School of Epidemiology.
Last edited by MickG0105; 1st Feb 2020 at 09:02. Reason: Spelling
In epidemiology super-spreaders are not a hypothesis; they are known and documented phenomenon dating back to 'Typhoid Mary'. Super spreader events have been documented in both major previous coronavirus outbreaks - SARS and MERS.
Have a read of Stein's 2010 'Super-spreaders in infectious diseases' or Chun's 2016 'Understanding and Modeling the Super-spreading Events of the Middle East Respiratory Syndrome Outbreak in Korea' if you want to inform yourself.
If you want to argue the toss take it up with your local School of Epidemiology.
Have a read of Stein's 2010 'Super-spreaders in infectious diseases' or Chun's 2016 'Understanding and Modeling the Super-spreading Events of the Middle East Respiratory Syndrome Outbreak in Korea' if you want to inform yourself.
If you want to argue the toss take it up with your local School of Epidemiology.
What I don�t understand is why VIR are still operating LHR-PVG when there�s a do not travel notice out from FCO?
When SSH closed, airlines were forced to repatriate passengers back at their cost?
When SSH closed, airlines were forced to repatriate passengers back at their cost?
Authorities have been very slow off the mark.
There was a reason why China implemented extraordinary measures several weeks ago. They understood the consequences of exponential growth.
I have been following this guy for the last week. His model has predicted the outcome very accurately so far.
https://twitter.com/matt_barrie
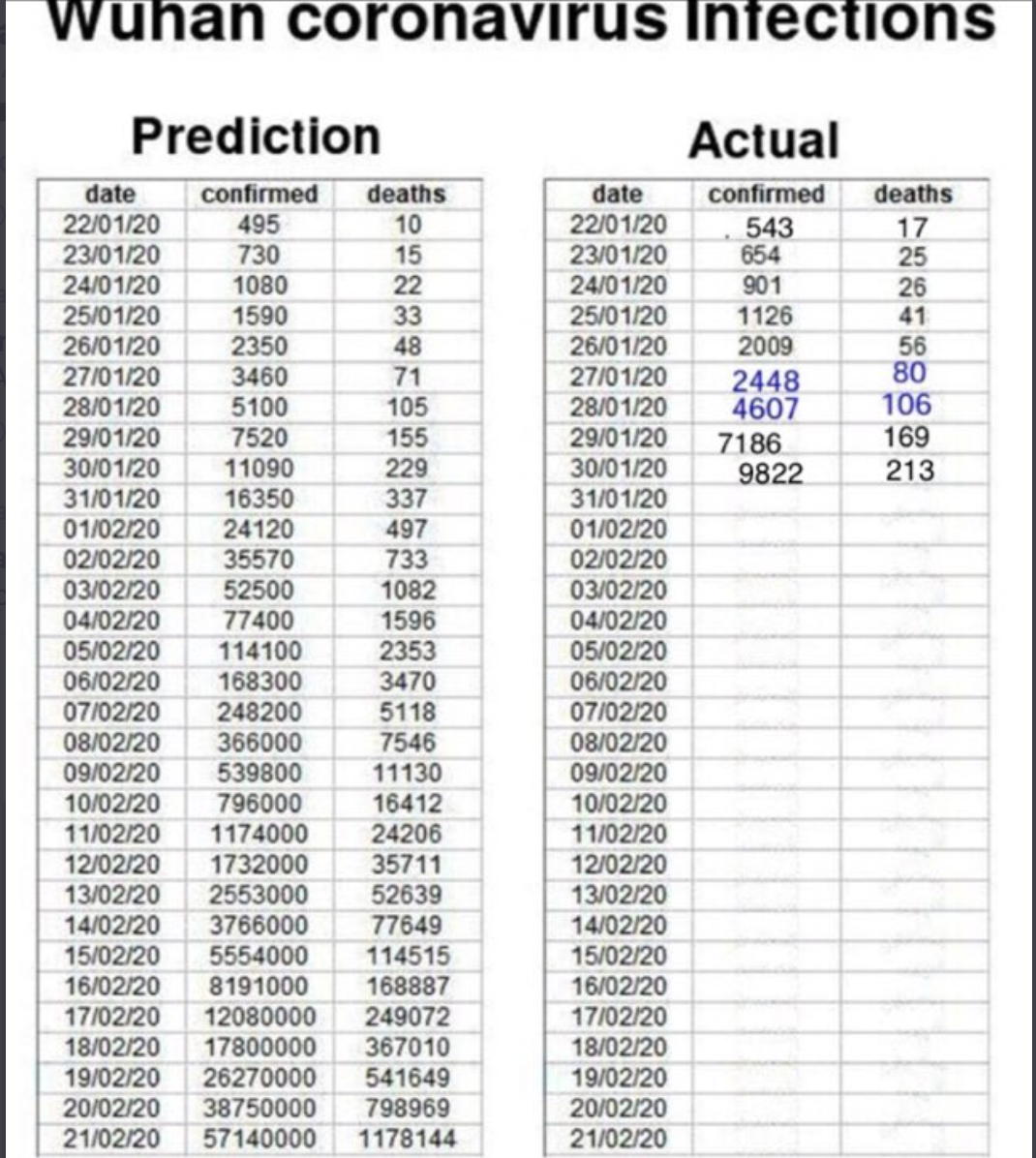
Understand also that China has cut back testing due to a shortage of test kits.
As of earlier today
11,860 conformed cases
17,988 additional suspected cases
259 died
243 recovered (fewer recovered than have died)

https://bnonews.com/index.php/2020/0...navirus-cases/
There was a reason why China implemented extraordinary measures several weeks ago. They understood the consequences of exponential growth.
I have been following this guy for the last week. His model has predicted the outcome very accurately so far.
https://twitter.com/matt_barrie
Understand also that China has cut back testing due to a shortage of test kits.
As of earlier today
11,860 conformed cases
17,988 additional suspected cases
259 died
243 recovered (fewer recovered than have died)
https://bnonews.com/index.php/2020/0...navirus-cases/
Last edited by slats11; 1st Feb 2020 at 09:36.
Why include Hong Kong, Normanton? At last glance, Hong Kong & Australia had a broadly similar number of confirmed cases. Hong Kong imposed restricted entry access to mainland Chinese visitors several days ago; Australia has only just commenced it. Your chances of catching the virus here in Hong Kong are probably not much different to your risk in the metropolitan parts of Australia.
Why include Hong Kong, Normanton? At last glance, Hong Kong & Australia had a broadly similar number of confirmed cases. Hong Kong imposed restricted entry access to mainland Chinese visitors several days ago; Australia has only just commenced it. Your chances of catching the virus here in Hong Kong are probably not much different to your risk in the metropolitan parts of Australia.
I thought that Hong Kong is China.
Join Date: Jun 2010
Location: Sydney
Age: 41
Posts: 483
Likes: 0
Received 0 Likes
on
0 Posts
Why include Hong Kong, Normanton? At last glance, Hong Kong & Australia had a broadly similar number of confirmed cases. Hong Kong imposed restricted entry access to mainland Chinese visitors several days ago; Australia has only just commenced it. Your chances of catching the virus here in Hong Kong are probably not much different to your risk in the metropolitan parts of Australia.
Originally Posted by MickG0105 [img]images/buttons/viewpost.gif[/img]
https://www1.health.gov.au/internet/...models-2.2.htm
The basic reproduction number (R0) is the reproduction number when there is no immunity from past exposures or vaccination, nor any deliberate intervention in disease transmission.
R0 is a theoretical expression of the infectivity of the organism per se. Measles virus has a high R0, hence we immunise against it and there are no pandemics (although isolated outbreaks where vaccination rates are lower). Influenza has a fairly low R0, but spreads quickly as the virus mutates (changes) each year meaning little immunity, because the vaccine is only partly protective, and because many people chose not to vaccinate.
The latest paper suggests this virus has a R0 of at least 4. That is a disaster with no immunity, and a vaccine perhaps 12 months away.
https://www.worldometers.info/coronavirus/#repro
Finally, the fatality rate for 'flu is very low - perhaps 0.01%
The fatality rate for this is at least 2%, but is almost certainly higher.
Early during an epidemic, the fatality rate is lowered by the rapid growth of newly infected people (who have not yet had time to die).
https://www.worldometers.info/coronavirus/#repro
Note that the mortality within Wahun city (the epicentre where the data is more robust as it has been going longer), the mortality is already 5.5%
During the SARS outbreak (another coronavirus), initial data suggested a mortality less than 4%. This was revised to 6-7%. Then revised to 12-14%. People remember that it ended at 12%, but forget early data suggested < 4%.
With MERS (a much smaller coronavirus outbreak), the mortality was 35%. But the current coronavirus outbreak is already orders of magnitude larger than MERS.
And that is why we have belatedly closed the border to Chinese visitors. And that is why it was too little too late
R0 is not a necessarily good indicator of pandemicity. Measles has an R0 of 12-16, seasonal influenza has an R0 of 1.3.
The basic reproduction number (R0) is the reproduction number when there is no immunity from past exposures or vaccination, nor any deliberate intervention in disease transmission.
R0 is a theoretical expression of the infectivity of the organism per se. Measles virus has a high R0, hence we immunise against it and there are no pandemics (although isolated outbreaks where vaccination rates are lower). Influenza has a fairly low R0, but spreads quickly as the virus mutates (changes) each year meaning little immunity, because the vaccine is only partly protective, and because many people chose not to vaccinate.
The latest paper suggests this virus has a R0 of at least 4. That is a disaster with no immunity, and a vaccine perhaps 12 months away.
https://www.worldometers.info/coronavirus/#repro
How contagious is the Wuhan Coronavirus? (Ro)
The attack rate or transmissibility (how rapidly the disease spreads) of a virus is indicated by its reproductive number (Ro, pronounced R-nought or r-zero), which represents the average number of people who will catch the disease from a single infected person.
R0 is the number of uninfected people each infected person will infect on average. While R0 > 1, outbreak increases. Eventually something happens - quarantine, vaccine, or simply most people have already been exposed and can't be re-infected. R0 falls below 1, and the outbreak starts to recede.
A more recent study is indicating a Ro as high as 4.08.[[url=https://www.worldometers.info/coronavirus/#ref-22]22]. This value substantially exceeds WHO's estimate (made on Jan. 23) of between 1.4 and 2.5[[url=https://www.worldometers.info/coronavirus/#ref-13]13], and is also higher than recent estimates between 3.6 and 4.0 and between 2.24 to 3.58 [[url=https://www.worldometers.info/coronavirus/#ref-23]23]. Preliminary studies had estimated Ro to be between 1.5 and 3.5 [[url=https://www.worldometers.info/coronavirus/#ref-5]5][[url=https://www.worldometers.info/coronavirus/#ref-6]6][[url=https://www.worldometers.info/coronavirus/#ref-7]7]
Based on these numbers, on average every case of the Novel Coronavirus would create 3 to 4 new cases.
An outbreak with a reproductive number of below 1 will gradually disappear.
For comparison, the Ro for the common flu is 1.3 and for SARS it was 2.0.
R0 is the number of uninfected people each infected person will infect on average. While R0 > 1, outbreak increases. Eventually something happens - quarantine, vaccine, or simply most people have already been exposed and can't be re-infected. R0 falls below 1, and the outbreak starts to recede.
A more recent study is indicating a Ro as high as 4.08.[[url=https://www.worldometers.info/coronavirus/#ref-22]22]. This value substantially exceeds WHO's estimate (made on Jan. 23) of between 1.4 and 2.5[[url=https://www.worldometers.info/coronavirus/#ref-13]13], and is also higher than recent estimates between 3.6 and 4.0 and between 2.24 to 3.58 [[url=https://www.worldometers.info/coronavirus/#ref-23]23]. Preliminary studies had estimated Ro to be between 1.5 and 3.5 [[url=https://www.worldometers.info/coronavirus/#ref-5]5][[url=https://www.worldometers.info/coronavirus/#ref-6]6][[url=https://www.worldometers.info/coronavirus/#ref-7]7]
Based on these numbers, on average every case of the Novel Coronavirus would create 3 to 4 new cases.
An outbreak with a reproductive number of below 1 will gradually disappear.
For comparison, the Ro for the common flu is 1.3 and for SARS it was 2.0.
Finally, the fatality rate for 'flu is very low - perhaps 0.01%
The fatality rate for this is at least 2%, but is almost certainly higher.
Early during an epidemic, the fatality rate is lowered by the rapid growth of newly infected people (who have not yet had time to die).
https://www.worldometers.info/coronavirus/#repro
Note that the mortality within Wahun city (the epicentre where the data is more robust as it has been going longer), the mortality is already 5.5%
During the SARS outbreak (another coronavirus), initial data suggested a mortality less than 4%. This was revised to 6-7%. Then revised to 12-14%. People remember that it ended at 12%, but forget early data suggested < 4%.
With MERS (a much smaller coronavirus outbreak), the mortality was 35%. But the current coronavirus outbreak is already orders of magnitude larger than MERS.
And that is why we have belatedly closed the border to Chinese visitors. And that is why it was too little too late
Last edited by slats11; 1st Feb 2020 at 10:13. Reason: clarification
"One bright spot is the Chinese habit of wearing a mask when ill to prevent the unchecked cloud of virus in every exhalation. That particular habit is something that the government would be wise to promote on TV etc"
no evidence it helps at all - far better to wash your hands regularly
no evidence it helps at all - far better to wash your hands regularly
https://www.ijidonline.com/article/S...008-4/fulltext
You do understand that R0 is essentially population/demographic/behaviour specific, right? That's why we're seeing a range of R0s. R0 will inevitably be higher in the nascent population, that's why the estimate for Wuhan is at the high end of the range.
As I said in a separate post, R0 says nothing about speed of spread. And R0 says nothing about the means of contagion or the vector.
In other words, as I said right from the set to, R0 is not necessarily a good indicator of pandemicity. R0 is not destiny, it is not the same as R (actual transmission rate). It is a measure of a disease’s potential.
No, it is not a disaster because immunity and vaccines are not the only method of containing or curtailing the spread of a disease.
We know that 2019-nCov appears to spread the same way as SARS, that is, close person-to-person contact by respiratory droplet spread. And we know that basic infection control practices, such as hand washing, are very effective in containing that sort of spread. It is worth noting that SARS wasn't contained through the deployment of a vaccine (the SARS vaccine was never deployed), SARS was contained through the deployment of basic infection control practices.
And while we're remembering things, remember that it took about five months for the WHO to declare SARS a global health threat. It's taken them one month this time around. China has reacted faster and more effectively. The global containment and counter-effort has been deployed faster and more effectively.
Do you understand what an 'order of magnitude' is?
The number of 2019-nCoV cases (~12,000) is currently not yet one (singular) order of magnitude larger than the number of MERS cares (~2,000).
Last edited by MickG0105; 1st Feb 2020 at 12:25. Reason: Grammar
Originally Posted by slats11 [img]images/buttons/viewpost.gif[/img]
The basic reproduction number (R0) is the reproduction number when there is no immunity from past exposures or vaccination, nor any deliberate intervention in disease transmission.
Yeah, thanks, you're telling me nothing about R0 I don't already know.
The basic reproduction number (R0) is the reproduction number when there is no immunity from past exposures or vaccination, nor any deliberate intervention in disease transmission.
Yeah, thanks, you're telling me nothing about R0 I don't already know.
Originally Posted by slats11 [img]images/buttons/viewpost.gif[/img]
That is a disaster with no immunity, and a vaccine perhaps 12 months away.
No, it is not a disaster because immunity and vaccines are not the only method of containing or curtailing the spread of a disease.
That is a disaster with no immunity, and a vaccine perhaps 12 months away.
No, it is not a disaster because immunity and vaccines are not the only method of containing or curtailing the spread of a disease.
SARS was contained through the deployment of basic infection control practices.
2019-nCoV has already infected far more people in a little over a month than did SARS in 7 months.
Cities were not locked down and borders closed for SARS.
In the city of Huanggang, people are housebound and 1 family member is allowed outside even 2nd day to get necessities. That didn't happen with SARS.
But if it makes you happier to say it is SARS...... then that's fine.
I don't which people remember SARS having a mortality rate of 12%?! There were 8,098 recorded cases resulting in 774 deaths for a mortality rate of 9.55%, or at least that's the I remember it.
May 7, 2003 (CIDRAP News) – The World Health Organization (WHO) today estimated the overall fatality rate for SARS (severe acute respiratory syndrome) patients at 14% to 15%, significantly higher than previous estimates. The agency estimated the rate for people older than 64 years to be more than 50%.
In the early stages of the SARS epidemic, health officials estimated the mortality rate at less than 4%. More recently, officials have cited rates in the 6% to 7% range. Today's SARS figures from the WHO—6,903 cumulative cases and 495 deaths—point to a case-fatality ratio of 7.2%. But WHO officials note that this calculation underestimates the rate, since some currently ill patients will die of the disease.
WHO officials observed that calculating the case-fatality ratio for a disease outbreak is difficult while the outbreak is still evolving. The true ratio cannot be determined until the outbreak is over, when the total numbers of deaths and recoveries are known.
In the early stages of the SARS epidemic, health officials estimated the mortality rate at less than 4%. More recently, officials have cited rates in the 6% to 7% range. Today's SARS figures from the WHO—6,903 cumulative cases and 495 deaths—point to a case-fatality ratio of 7.2%. But WHO officials note that this calculation underestimates the rate, since some currently ill patients will die of the disease.
WHO officials observed that calculating the case-fatality ratio for a disease outbreak is difficult while the outbreak is still evolving. The true ratio cannot be determined until the outbreak is over, when the total numbers of deaths and recoveries are known.
The final SARS mortality is still disputed due to concerns about the completeness of the mainland Chinese dataset. Maybe it was 10%, maybe 12, maybe 14. It was almost certainly between the range of 10-14% anyway.
MERS was accepted to be 35%
This is the 3rd recent coronavirus outbreak. To accept the current 2% figure is very optimistic. Especially when the data from Wuhan (where the epidemic has been unfolding longer) suggests a mortality of 5.5% (and this too will go up).
Do you understand what an 'order of magnitude' is?
So MERS was perhaps 2,494 (858 deaths, fatality 35%)
It is estimated that the number of infected in Wuhan alone could be greater than 75,000. That was the calculation on Tuesday - with continued exponential growth in the 4 days since then.
https://www.scmp.com/news/china/arti...hubei-province
Thats just Wuhan city. What about the rest of the province? What about the rest of China?
You realise they have run out of test kits in Wuhan
You realise Indonesia doesn't have a reported case - because it currently has no testing.
So Mick, by what order of magnitude do you believe 2019-nCoV exceeds MERS? Because I suspect it is close to 2.
"One bright spot is the Chinese habit of wearing a mask when ill to prevent the unchecked cloud of virus in every exhalation. That particular habit is something that the government would be wise to promote on TV etc"
no evidence it helps at all - far better to wash your hands regularly
no evidence it helps at all - far better to wash your hands regularly
For R0 = β * c * D, where
β = transmission probability
c = number of contacts
D = average time spent infectious
he is using constants.
And we know that the real world doesn't work that way. As soon as health authorities understand what they're dealing with and start implementing appropriate infection control practices, β declines. Same same with c; simple population awareness, public infection control practices, movement restrictions and quarantines drive the number of contacts down. As a result R (actual) declines over time.
Last edited by MickG0105; 1st Feb 2020 at 21:28. Reason: Correction to R v R0
Lets hope the model diverges over time.
But have a read of that Lancet paper calculating 75k cases in Wuhan as of Tuesday 28th.
And lets see what happens when it gets loose in India. Because if China can't control it, what chance India?
But have a read of that Lancet paper calculating 75k cases in Wuhan as of Tuesday 28th.
And lets see what happens when it gets loose in India. Because if China can't control it, what chance India?
Last edited by slats11; 1st Feb 2020 at 13:18. Reason: spelling
short flights long nights
I am starting to think �conspiracy theory�
Everything was good.. until it was not
Flights from Australia could continue .. until they could not.
Flights from China to Australia were fine... until they were not.
Something is not adding up... a lot of knee jerking? Or we know something you don�t?
Everything was good.. until it was not
Flights from Australia could continue .. until they could not.
Flights from China to Australia were fine... until they were not.
Something is not adding up... a lot of knee jerking? Or we know something you don�t?

I suspect that you are well informed about R and R0. But my point was that other readers may be falsely reassured by the fact measles is not out of control despite its R0 of 14, and the explanation for this is immunisation.
OK. Lets revisit this debate in a week
Sure. But that hasn't worked this time has it?
2019-nCoV has already infected far more people in a little over a month than did SARS in 7 months.
Cities were not locked down and borders closed for SARS.
In the city of Huanggang, people are housebound and 1 family member is allowed outside even 2nd day to get necessities. That didn't happen with SARS.
But if it makes you happier to say it is SARS...... then that's fine.
Estimates of SARS death rates revised upward | CIDRAP
The point is the mortality rate appears to increases over time due to the lag between getting sick and dying.
The final SARS mortality is still disputed due to concerns about the completeness of the mainland Chinese dataset. Maybe it was 10%, maybe 12, maybe 14. It was almost certainly between the range of 10-14% anyway.
MERS was accepted to be 35%
This is the 3rd recent coronavirus outbreak. To accept the current 2% figure is very optimistic. Especially when the data from Wuhan (where the epidemic has been unfolding longer) suggests a mortality of 5.5% (and this too will go up).
Umm, do you add a zero? Is that right?
So MERS was perhaps 2,494 (858 deaths, fatality 35%)
It is estimated that the number of infected in Wuhan alone could be greater than 75,000. That was the calculation on Tuesday - with continued exponential growth in the 4 days since then.
https://www.scmp.com/news/china/arti...hubei-province
Thats just Wuhan city. What about the rest of the province? What about the rest of China?
You realise they have run out of test kits in Wuhan
You realise Indonesia doesn't have a reported case - because it currently has no testing.
So Mick, by what order of magnitude do you believe 2019-nCoV exceeds MERS? Because I suspect it is close to 2.
OK. Lets revisit this debate in a week
Sure. But that hasn't worked this time has it?
2019-nCoV has already infected far more people in a little over a month than did SARS in 7 months.
Cities were not locked down and borders closed for SARS.
In the city of Huanggang, people are housebound and 1 family member is allowed outside even 2nd day to get necessities. That didn't happen with SARS.
But if it makes you happier to say it is SARS...... then that's fine.
Estimates of SARS death rates revised upward | CIDRAP
The point is the mortality rate appears to increases over time due to the lag between getting sick and dying.
The final SARS mortality is still disputed due to concerns about the completeness of the mainland Chinese dataset. Maybe it was 10%, maybe 12, maybe 14. It was almost certainly between the range of 10-14% anyway.
MERS was accepted to be 35%
This is the 3rd recent coronavirus outbreak. To accept the current 2% figure is very optimistic. Especially when the data from Wuhan (where the epidemic has been unfolding longer) suggests a mortality of 5.5% (and this too will go up).
Umm, do you add a zero? Is that right?
So MERS was perhaps 2,494 (858 deaths, fatality 35%)
It is estimated that the number of infected in Wuhan alone could be greater than 75,000. That was the calculation on Tuesday - with continued exponential growth in the 4 days since then.
https://www.scmp.com/news/china/arti...hubei-province
Thats just Wuhan city. What about the rest of the province? What about the rest of China?
You realise they have run out of test kits in Wuhan
You realise Indonesia doesn't have a reported case - because it currently has no testing.
So Mick, by what order of magnitude do you believe 2019-nCoV exceeds MERS? Because I suspect it is close to 2.
And yes, regarding orders of magnitude, you add a zero on the right or move the decimal place left. So 200,000 is two orders of magnitude higher than 2,000. We're not there yet by any stretch of the imagination.
The WHO Collaborating Centre for Infectious Disease Epidemiology and Control puts the total infections for Wuhan at less than 5,000. The Northeastern University's Laboratory for the Modeling of Biological and Socio-technical Systems predicts Wuhan might be as high as 25,000. WHO CCIDEC puts total infections elsewhere in China at less than 10,000. The total China figure outside of Wuhan might be higher but not by the same factor as Wuhan so maybe 30,000.
It's early days but we haven't seen any deaths outside of China yet. So, glass half full. And China being China, and having previously dealt with SARS, is probably the only country in the world outside of maybe North Korea that can apply extraordinarily stringent public health measures and restrictions. So, we'll see.
A wild card is seasonality. We don't have any real feel for whether 2019-nCoV has a seasonality component.
Any old how, let's just revisit this in a week and see where we stand. And let's stick to WHO confirmed cases and deaths.
Oh, and as an addendum, while we're wringing out hands over this, 2019/2020 seasonal influenza in the US has killed about 8,000 people (at the rate of 250 people dying of it per day for the week between 16 - 22 January).
Last edited by MickG0105; 1st Feb 2020 at 13:52. Reason: Seasonality factor added, US flu stats