


UK Air Ambulances having it off???

The SAR posters will attempt to shoot me down, telling me how many 'successful' transfers they have undertaken, but the level of medical care will always be compromised

You are absolutely correct. For 20 years, faced with a free transfer from SAR or paying a couple of thousand pounds for a dedicated system, hospital managers took the free option. Basically they refused to pay until there was no alternative.
What you are doing is indeed better in many cases than no transfer at all. However the taxpayer is suffering a bigger hit and patient care cannot be as good.
The need for transfers has fallen due to developments in intensive care and to a degree the destruction of specialised units by politicians. Nevertheless I believe some 300 transfers a year do not occur because the NHS wants to save money. Some of these go by road to the potential detriment of the patient. Others simply don't happen. England and Wales.would be adequately covered by two helicopters and one fixed wing (ignoring maintenance)
What you are doing is indeed better in many cases than no transfer at all. However the taxpayer is suffering a bigger hit and patient care cannot be as good.
The need for transfers has fallen due to developments in intensive care and to a degree the destruction of specialised units by politicians. Nevertheless I believe some 300 transfers a year do not occur because the NHS wants to save money. Some of these go by road to the potential detriment of the patient. Others simply don't happen. England and Wales.would be adequately covered by two helicopters and one fixed wing (ignoring maintenance)
TC
have been around but so busy in the past 4 months haven't had time to do much else ! My concern over the whole AA thing is they seem to be getting away from the concept of getting someone to hospital and best medical support asap. I know the mil called it the golden hour and they now take a whole trauma team to the casualty in Afgan, but that is for the guys and gals being blown up. It seems that AA's over here are going down the same way, why ? Don't see too many people being blown up over here. So why have a very very expensive machine now being twin pilot IFR capable when a much cheaper and probably more efficient system with perhaps a greater number of machines could be utilised otherwise we will be seeing CH47's with a mini hospital in the back being deployed
I would love to know how many shouts end up being needed ? What I mean is the patient would have either died or been seriously impaired for the rest of their life if it wasn't for a helicopter. I can remember one incident with a broken leg on a rugby field where we got an air ambulance, great for the kids to see but !!!!!!!!!!!!
have been around but so busy in the past 4 months haven't had time to do much else ! My concern over the whole AA thing is they seem to be getting away from the concept of getting someone to hospital and best medical support asap. I know the mil called it the golden hour and they now take a whole trauma team to the casualty in Afgan, but that is for the guys and gals being blown up. It seems that AA's over here are going down the same way, why ? Don't see too many people being blown up over here. So why have a very very expensive machine now being twin pilot IFR capable when a much cheaper and probably more efficient system with perhaps a greater number of machines could be utilised otherwise we will be seeing CH47's with a mini hospital in the back being deployed
I would love to know how many shouts end up being needed ? What I mean is the patient would have either died or been seriously impaired for the rest of their life if it wasn't for a helicopter. I can remember one incident with a broken leg on a rugby field where we got an air ambulance, great for the kids to see but !!!!!!!!!!!!
Join Date: Oct 2012
Location: UK
Posts: 11
Likes: 0
Received 0 Likes
on
0 Posts
My concern over the whole AA thing is they seem to be getting away from the concept of getting someone to hospital and best medical support asap. I know the mil called it the golden hour and they now take a whole trauma team to the casualty in Afgan, but that is for the guys and gals being blown up. It seems that AA's over here are going down the same way, why ? Don't see too many people being blown up over here.
It's also worth remembering that the concept of taking extended care to the patient, in addition to taking the patient to a definitive care centre, has been evident in civ practice for a number of years and has been shown to work. London HEMS is a prime example.
Apologies for the thread drift.
The improvements in Afghanistan have in the main been driven by money. . For example every casualty is met by a CT scanner and consultant radiologist. The ability to evacuate to the UK etc etc. And the money to train every member of the medical ream for weeks before deployment whereas in the UK managers wont stop clinical work for training.
The prehospital team has been improved by including a doctor, but this really just follows the Sheffield study which showed the only benefit they could demonstrate from HEMS was the occasional medical intervention in the field if the helicopter carried a doctor.
The main difference IMHO is that in the theatre of war you get sadly recurrent major trauma and in most cases an embedded first responder who can task HEMS. In civilian scenarios many patients have quite minor injuries and there is a political requirement to decide the response at notification with minimal information, so most HEMS missions do not improve outcome
This is as mentioned off thread as the issue is whether we need massive complex machines. There is no evidence they will improve patient outcome.
The prehospital team has been improved by including a doctor, but this really just follows the Sheffield study which showed the only benefit they could demonstrate from HEMS was the occasional medical intervention in the field if the helicopter carried a doctor.
The main difference IMHO is that in the theatre of war you get sadly recurrent major trauma and in most cases an embedded first responder who can task HEMS. In civilian scenarios many patients have quite minor injuries and there is a political requirement to decide the response at notification with minimal information, so most HEMS missions do not improve outcome
This is as mentioned off thread as the issue is whether we need massive complex machines. There is no evidence they will improve patient outcome.
Is there any information out there that actually breaks down the number of missions that actually have saved a life instead of backing up an under resourced land ambulance. I get the impression an AA is launched for relatively minor injuries. Certainly a CP of an AA gives me that impression
Join Date: Sep 2006
Location: 'oop North
Posts: 156
Likes: 0
Received 0 Likes
on
0 Posts
I get the impression an AA is launched for relatively minor injuries. Certainly a CP of an AA gives me that impression
Then perhaps that AA should be taking a good look at their launch protocols and how they are applied...
Then perhaps that AA should be taking a good look at their launch protocols and how they are applied...
The only proper audit of 'lives saved' is some 20 years old and called the Sheffield study. It demonstrated that HEMS with doctor as in London saved 1-5 lives a year at a cost then equivalent to heart transplantation. This would now be more like three times a heart transplant. It failed to demonstrate lives saved for paramedic HEMS. Sadly no service has produced any peer reviewed data in the mainstream medical literature that I am aware of - happy to be proved wrong
HEMS do not task themselves. The decision to launch is taken by the ambulance service. Some services have a specific controller who oversees this. Some services will task in order to meet government targets on arrival time - so they may send a helicopter to a minor problem because they have no land based ambulances or because the land based service would take longer than the target time they have to meet. I know of one service that uses or has used midwives and first aiders to meet the targets, so if you cut your finger you may get the local butcher with a bandage or a twin engined IFR helo solely on the basis of what is available to the controller. Welcome to the logic of the NHS
HEMS do not task themselves. The decision to launch is taken by the ambulance service. Some services have a specific controller who oversees this. Some services will task in order to meet government targets on arrival time - so they may send a helicopter to a minor problem because they have no land based ambulances or because the land based service would take longer than the target time they have to meet. I know of one service that uses or has used midwives and first aiders to meet the targets, so if you cut your finger you may get the local butcher with a bandage or a twin engined IFR helo solely on the basis of what is available to the controller. Welcome to the logic of the NHS
Join Date: Aug 2004
Location: London, UK
Posts: 226
Likes: 0
Received 0 Likes
on
0 Posts
other article from Torygraph
More developments in salaries/transparency:
Analysis: Fat cats? The bigger picture of senior salaries | Third Sector
And from the tabloids:
Charities set to be forced to be more open about how much they pay their top executives - Telegraph
Analysis: Fat cats? The bigger picture of senior salaries | Third Sector
And from the tabloids:
Charities set to be forced to be more open about how much they pay their top executives - Telegraph
Join Date: Aug 2001
Location: Cornwall
Age: 75
Posts: 1,307
Likes: 0
Received 0 Likes
on
0 Posts
Dispatch - yes or no
At the risk of a little thread drift those who have contributed to this thread may like to read about how we dealt with the very first UK AA's dispatch protocols.
I am giving a series of talks as an AA fund raiser and book promotion and produced a booklet to accompany them. This describes how the project came about and is available as a download from the blog section of my website and I think that some parts of the tale will surprise you. Visit Geoff Newman - ignore the book sales part, go to the blog and download the booklet.
In those days we faced a different set of problems and could only dream of being able to raise the funds raised across the UK today. Imagine what it was like starting off with not a single penny in the pot.
G.
I am giving a series of talks as an AA fund raiser and book promotion and produced a booklet to accompany them. This describes how the project came about and is available as a download from the blog section of my website and I think that some parts of the tale will surprise you. Visit Geoff Newman - ignore the book sales part, go to the blog and download the booklet.
In those days we faced a different set of problems and could only dream of being able to raise the funds raised across the UK today. Imagine what it was like starting off with not a single penny in the pot.
G.
Last edited by Geoffersincornwall; 14th Dec 2013 at 18:06.
Join Date: Aug 2001
Location: Cornwall
Age: 75
Posts: 1,307
Likes: 0
Received 0 Likes
on
0 Posts
Thanks
Thanks to the large number of folk that downloaded my booklet and gave me valuable feedback. If there are any more questions about that fascinating period please don't hesitate to PM me.
G.
PS. I'm particularly interested in discussing the approach we had to dispatch criteria compared to what we see today.
G.
PS. I'm particularly interested in discussing the approach we had to dispatch criteria compared to what we see today.
Last edited by Geoffersincornwall; 22nd Dec 2013 at 17:13.
Guest
Join Date: Feb 2003
Posts: 210
Likes: 0
Received 0 Likes
on
0 Posts
despatch
I think that the secondary mission (surveyed site -> hospital) is very much underused these days due to a) the time it takes to achieve patient to hospital b) the cost c) the aims & ethos of the charity.
Join Date: Aug 2001
Location: Cornwall
Age: 75
Posts: 1,307
Likes: 0
Received 0 Likes
on
0 Posts
Delta Ng - Time to hospital
Are you saying that the road situation is now such that an emergency vehicle can be 'returned-to-service' in an acceptable time frame?
Maybe that's the case in some areas - that's progress. Maybe not so easy to achieve in the more difficult rural areas.
In which case is this business of 'policy' overshadowing the possibility of using the AA in it's role as 'force-multiplier'?
ie, being operated for the maximum benefit of the Ambulance Service as a whole.
Is there an argument therefore, in favour of a review of current dispatch criteria? Are we using the potential of the AA to its maximum?
G
Maybe that's the case in some areas - that's progress. Maybe not so easy to achieve in the more difficult rural areas.
In which case is this business of 'policy' overshadowing the possibility of using the AA in it's role as 'force-multiplier'?
ie, being operated for the maximum benefit of the Ambulance Service as a whole.
Is there an argument therefore, in favour of a review of current dispatch criteria? Are we using the potential of the AA to its maximum?
G
A few words about the AA approaches that I have come across.
Just yesterday I came across a project that is expected to bring more diagnostic capability to the flightsuit pocket of air ambulance medical staff.
One manager from a rural UK air ambulance district has been annoying some of his air ambulance colleagues from more populated areas by stating that the only valid reason for having an air ambulance is rural location and distance.
Norway has only six SAR helicopter bases but a network of 12 helicopter air ambulance bases (& 7 FW) with some enhanced capability and typically flying with pilot, doctor and paramedic (sometimes rescuer). The Doctor and Paramedic are trained to provide aircrewman services during different phases of the operations. One mode of operation is to insert a paramedic at the casualty's location, possibly using long-line, so that there is medical aid until the SAR helicopter arrives to extract with its winch. Getting help to the casualty's side in the minimum time seems to be given a very high priority and then extraction can take place when the appropriate resources are available.
Just yesterday I came across a project that is expected to bring more diagnostic capability to the flightsuit pocket of air ambulance medical staff.
One manager from a rural UK air ambulance district has been annoying some of his air ambulance colleagues from more populated areas by stating that the only valid reason for having an air ambulance is rural location and distance.
Norway has only six SAR helicopter bases but a network of 12 helicopter air ambulance bases (& 7 FW) with some enhanced capability and typically flying with pilot, doctor and paramedic (sometimes rescuer). The Doctor and Paramedic are trained to provide aircrewman services during different phases of the operations. One mode of operation is to insert a paramedic at the casualty's location, possibly using long-line, so that there is medical aid until the SAR helicopter arrives to extract with its winch. Getting help to the casualty's side in the minimum time seems to be given a very high priority and then extraction can take place when the appropriate resources are available.

Wonders will never cease. Is this the first instance of a UK HEMS charity being proven to be at fault? There are certainly many high profile charities with royal links who behave in similar fashion when it comes to the rule of law, just culture and bare bones proper procedure.
As we have said before one need not look far to find abuses of power and position amongst charities. Maybe Private Eye will start to dig further.
As we have said before one need not look far to find abuses of power and position amongst charities. Maybe Private Eye will start to dig further.
Join Date: Jul 2014
Location: United Kingdom
Posts: 7
Likes: 0
Received 0 Likes
on
0 Posts
I find it interesting that the �whistleblower� is making so much noise on this technicality over a CV inaccuracy, when the noise may cause the charity commission to happen across the ramifications of some of the decisions he made just before resigning, particularly where it comes to service capabilities/availability.

Doesn't say much for the integrity and quality of those charged with running such important charities - this sort of thing will make people hesitate to put money in the tin if they think it isn't being used properly.
The charities commission has made it considerably easier in recent times to check up on how your charity spends their money.
It ranges from the inefficient:
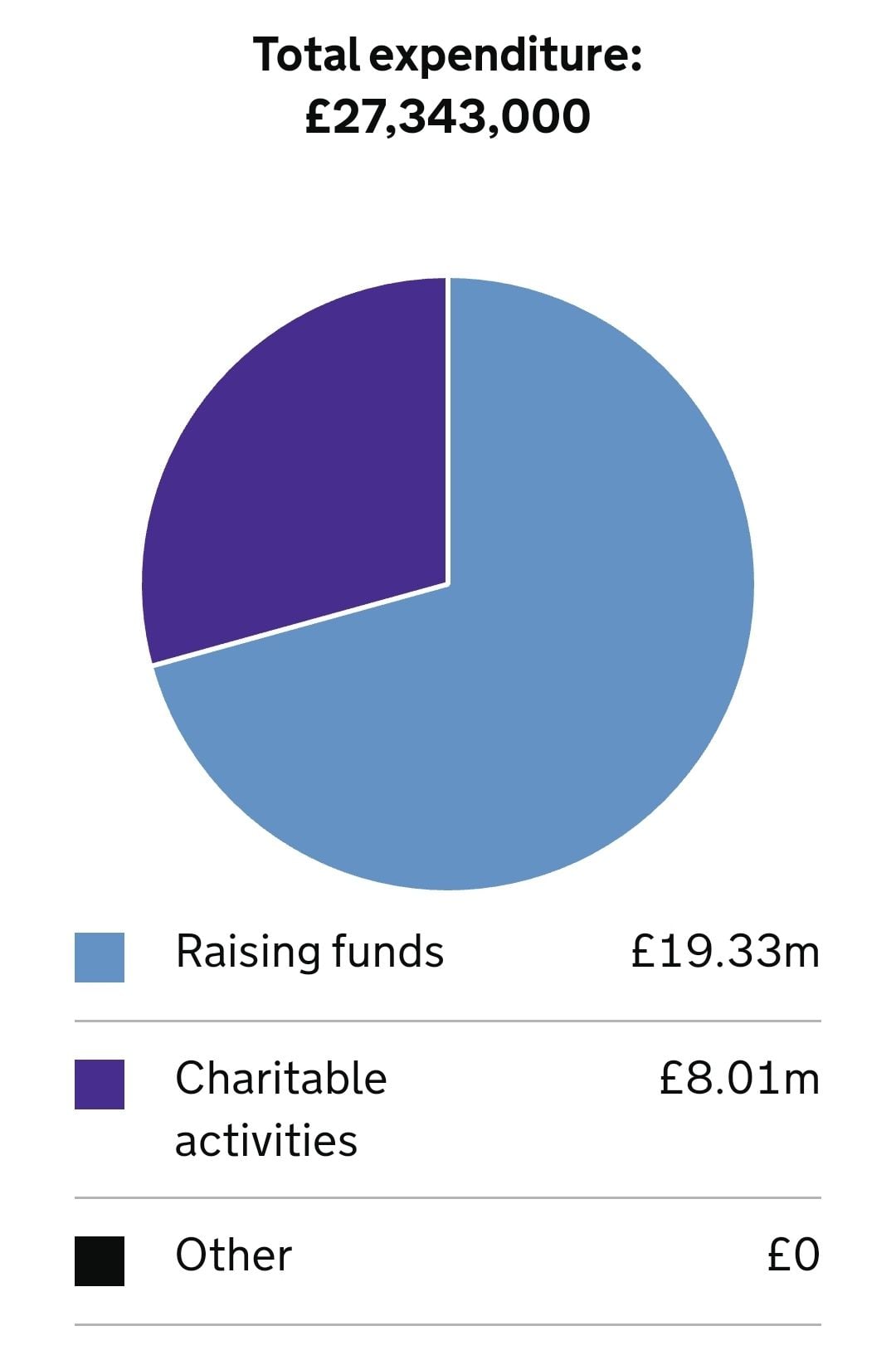
To the efficient:
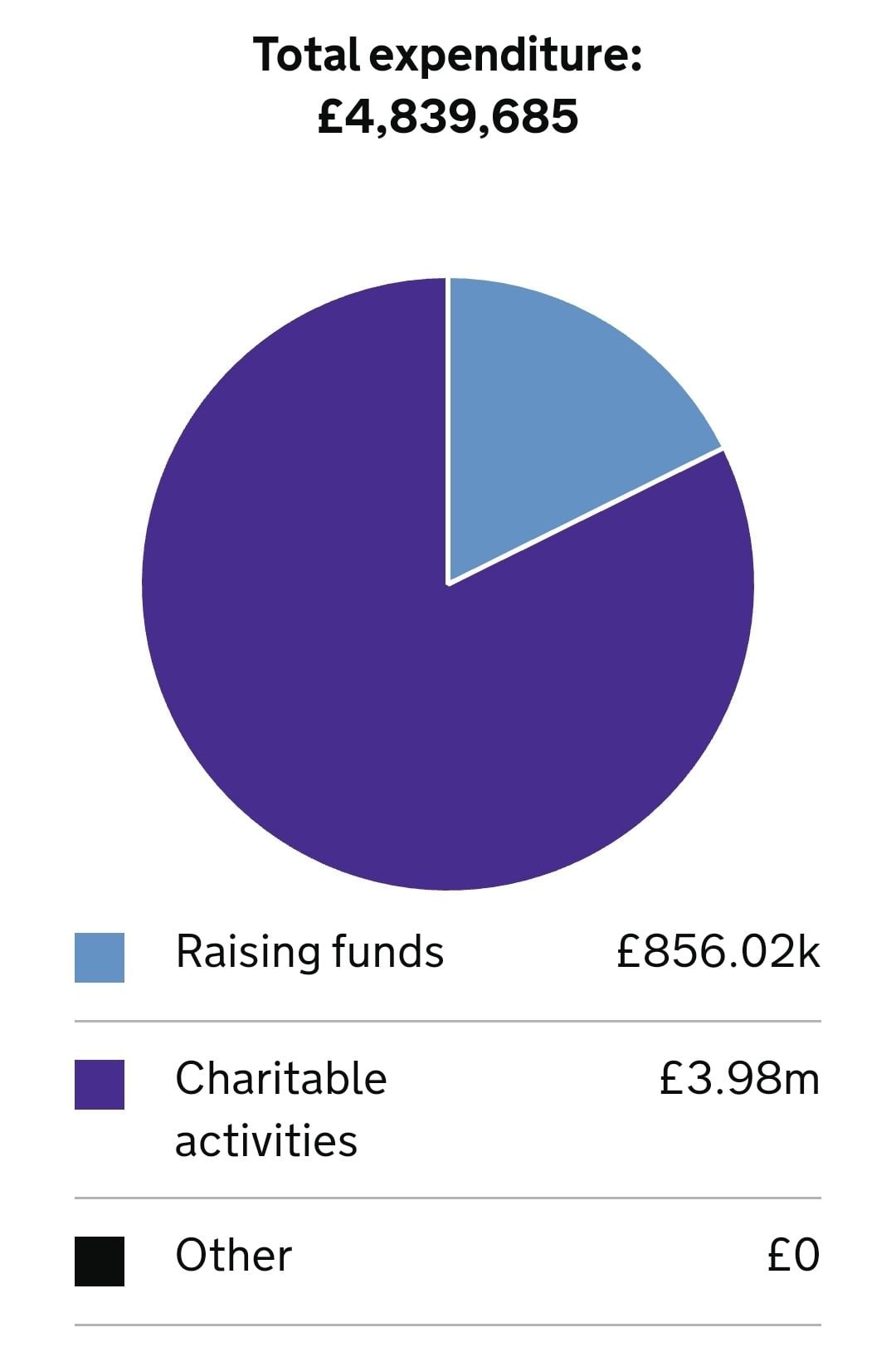
Take a moment to check what your local one is doing.
The following 2 users liked this post by gipsymagpie: